


Rectovaginal Fistula and Fecal Incontinence
WHEC Practice Bulletin and Clinical Management Guidelines for healthcare providers. Educational grant provided by Women's Health and Education Center (WHEC).
Childbirth is increasingly being recognized as commonly injuring the mother's anal sphincter complex. Fecal incontinence also appears to be associated with urinary incontinence and pelvic organ prolapse. The inability to control feces is also a devastating problem. Many people find this problem socially incapacitating and stay home, thus minimizing social contact to avoid an embarrassing situation. Rectovaginal fistula occurs when the tract is formed between rectum and vagina. Fecal incontinence is a relevant clinical issue for obstetricians and gynecologists, and requires compassion and emotional support on the part of the physician and healthcare team. This debilitating problem is underreported, but is thought to affect 2.2% of the general population. Women are 8 times more likely to have fecal incontinence than men, in age-controlled group. Although sphincter damage during vaginal delivery -- even in deliveries over an intact perineum -- may be clinically silent in most women, these women are at risk of developing overt fecal incontinence with subsequent deliveries, and with aging and its decompensating factors (1).
The purpose of this document is to understand etiology and management of rectovaginal fistula and fecal incontinence. Anal continence does not completely depend on intact sphincters; also important are intact neuromuscular function, including a functioning puborectalis muscle and pudendal nerve. This is supported by the fact that some women with sphincter lacerations remain continent. Anatomical knowledge of the anorectal canal is essential. Complications of anal sphincter laceration include anal incontinence, fecal urgency, perineal pain, and sexual dysfunction. Diagnostic studies, non-invasive therapies, and surgical management have all evolved in recent years. This has resulted in an improving outlook for women with this stigmatizing condition.
Etiology
There are many different causes of an abnormal epithelialized tract between the rectum and the vagina; the cause varies with the location of the fistula. Congenital rectovaginal fistulas are rare and are not discussed here.
Obstetric Trauma -- in developing countries obstructed labor is the most common cause of rectovaginal fistula. It can occur in association with vesicovaginal fistulas (2). Episiotomy is commonly performed in the practice of obstetrics. A rectal tear or anal sphincter disruption complicates up to one fourth of episiotomies. Although the majority of perineal injuries are successfully repaired at the time of the delivery, dehiscence of an episiotomy repair can occur and is associated with infection, abscess, fistula, or sphincter disruption. It is usually evident by day 3 or 4 after delivery. Midline episiotomy with resulting third- or fourth-degree laceration appears to be the greatest risk factor for development of a rectovaginal fistula. Mediolateral episiotomy, more common in British obstetric practice, causes fewer tears into the rectum when compared to midline incision. Rectovaginal fistulas following infection and dehiscence of an episiotomy most commonly occurs low in the rectovaginal septum but may extend much higher, especially in the case of a traumatic cloaca. Obstetric risk factors include: infant weighing more than 4,000 g; use of forceps; prolonged second stage of labor; midline episiotomy; occipito-posterior position and failed detection or suboptimal repair of anal sphincter injury at the time of vaginal delivery.
Iatrogenic -- rectovaginal fistula can follow any surgical procedure that involves the posterior wall of the vagina or the anterior wall of the rectum, such as rectocele repair or transanal excision of tumor. The fistula may result from a direct or unrecognized rectal injury, cautery, anastomotic leak, or infection (3).
Inflammatory Bowel Disease -- proctitis from inflammatory bowel disease (IBD), either ulcerative colitis or Crohn's disease, occurs up to 10% of patients with IBD. Most commonly, a rectovaginal fistula from Crohn's disease is located in the mid-rectovaginal septum. It can extend into the most distal aspect of the vagina or perineum. An anovaginal or rectovaginal fistula in Crohn's disease is more likely to result in proctectomy or disfunctioning stoma than anal Crohn's disease without rectovaginal fistula.
Infection -- the most common non-obstetric infection causing a rectovaginal fistula is a crypto-glandular abscess located in the anterior aspect of the anal canal. Extension of such an abscess into the vaginal wall can result in fistula formation. Other infections processes that may form fistula into vagina include lymphogranuloma venereum, tuberculosis, and Bartholin's abscess. Acquired rectovaginal fistula may be an early manifestation of human immunodeficiency virus (HIV) infection.
Endometriosis -- is rarely seen as a causative factor for rectovaginal fistula. Biopsy can confirm the diagnosis when it is suspected or needs to be differentiated with carcinoma of rectum or vagina.
Carcinoma and Lympho-proliferative Malignancy -- of rectum and vagina can cause rectovaginal fistula. Biopsy is done to make the diagnosis and should be ruled out if suspected before the repair.
Radiation -- rectovaginal fistulas develop in up to 6% of women following pelvic irradiation and are dependent on the radiation dosage. Rectovaginal fistulas are most commonly associated with radiation therapy for endometrial, cervical, and vaginal cancer. fistulas that present early during radiation therapy are more likely to be caused by destruction of the carcinoma, whereas fistulas caused by radiation injury may occur as late as 2 years after therapy. Late fistulas are commonly associated with a rectal stricture. It is critical to determine whether the rectovaginal fistula is caused by recurrent cancer in a patient with a history of genital carcinoma. This often requires examination under anesthesia with biopsies of the margins of the fistula. Rectovaginal fistulas caused by radiation injury are usually located in the mid-vagina or proximal vagina.
Evaluation and Physical Examination
A directed history helps indicate which diagnostic tests are most relevant. Establish severity and frequency of fecal incontinence, presence of fecal urgency, pad use, type of incontinence (solid, liquid, or gas), and presence of associated urinary incontinence and prolapse. Dietary habits (especially fiber intake) and chronic laxative use should be noted. Also note any history of abdomino-pelvic surgery, radiation, back injury, and neurologic disorders. In a low rectovaginal fistula, the rectal opening is located close to the dentate line, with the vaginal opening just inside the hymen. In a high rectovaginal fistula, the vaginal opening is near the cervix (or apex of the vagina in a post-hysterectomy patient); the communication into the intestinal tract may be located in either the sigmoid colon or rectum. A mid-rectovaginal fistula is found somewhere between the hymen and the cervix. It is important to determine the status of the anal sphincter mechanism when the patient's complaints are consistent with fecal seepage and before rectovaginal fistula repair. If a rectovaginal fistula is suspected, try retrograde filling of the rectum with 200 cc of dye-stained fluid (using a 50-cc catheter tip syringe), then observe vaginal extravasation.
Evaluation of anal sphincter -- conduct a digital rectal examination to assess the length and orientation of the anal canal, bulk of the perineal tissues, and tone of the anal sphincters, as well as to rule out a mass or impaction. Repeat digital examination with the patient bearing down to assess the squeeze pressures, movement of the puborectalis muscle, and extent of pelvic floor descent. Perform a vaginal exam to identify pelvic prolapse and presence or absence of rectovaginal fistula. Assess the anal wink (cutaneoanal contractile reflex) by stroking the skin surrounding the anus. Absence of a reflexive contraction of the external anal sphincter suggests nerve damage or spinal arc interruption. Inspect the perineum/perianal area for evidence of dermatitis, infection, fistula, hemorrhoids, and deformities of the anus. Ask the patient to bear down as you look for evidence of pelvic floor weakness and rectal prolapse. The pudendal nerve is susceptible to traction injury from childbirth and chronic straining. These findings are predominantly subjective and depend on operator experience. In general, they correlate poorly with objective measurements of sphincter pressures.
Diagnostic Strategies: Routine Endoanal Ultrasound, Manometry
It is important to bear in mind that continence depends on multiple physiologic mechanisms and therefore, no single diagnostic test yields positive results in all patients (4).
Endoanal Ultrasound -- has significantly changed the evaluation of fecal incontinence over the last decade. In women with fecal incontinence in whom obstetric injury is suspected, 90% have sonographic evidence of injury to one or both sphincters. The damage to internal anal sphincter and external anal sphincter can be easily seen by this technique. Endoanal ultrasound is regarded as superior to other diagnostic methods, with an accuracy of over 90% in detecting sphincter injuries, compared to 75% of manometry, 75% for electromyography (EMG), and 50% for clinical assessment. It is the simplest and least-invasive test to assess the structural integrity of the anal sphincters. It can also serve as a screening tool to detect occult sphincter injury following vaginal delivery, thus identifying women at high risk for future incontinence. Where endoanal ultrasound is unavailable, transperineal ultrasound may be an alternative option.
Anorectal Manometry -- it can detect functional weakness of sphincters that are anatomically intact by measuring sensation and squeeze pressures. Patients with intact sphincters but abnormal anal manometry findings may benefit from physical therapy and biofeedback aimed at increasing muscular function by stimulating the neuromuscular feedback loop. During manometry, the physician assesses maximum resting and squeeze-pressures of the anal canal, the rectoanal inhibitory reflex, rectal sensation, and rectal compliance using either water-perfused catheters, solid-state microtransducers, or air- or water-filled balloons. Normal values vary widely among institutions and are poorly standardized. Decreased resting pressure suggests isolated internal anal sphincter injury; decreased squeeze-pressure suggests external anal sphincter injury. Of all parameter, maximum squeeze pressure has the greatest sensitivity and specificity at a cut-off of 60 mm Hg in women.
Rectal Sensory Testing -- it is also useful in identifying patients who may benefit from biofeedback therapy, and detect afferent nerve injury as a contributing cause of incontinence. Biofeedback is unlikely to be useful in patients with a poor or absent sensation. In addition, for patients already involved in biofeedback, the test can assess rectal response to training and indicate rectal irritability or poor compliance. Rectal sensation is assessed by inflating a balloon in the rectum and recording the smallest volume of rectal distention for first detectable sensation (rectal sensory threshold), sensory urgency, and pain (maximum tolerable volume).
Ancillary Tests -- these are of limited benefit as screening tools, but may have utility in special circumstances. Electromyography (EMG) of the external anal sphincter and the pelvic floor muscles -- traditionally performed using needle electrodes or surface electrodes -- is helpful in delineating areas of sphincter injury by mapping the sphincter. However, much of this information is now obtained accurately by endoanal ultrasound, which has replaced needle EMG for most clinicians. Surface EMG is still useful for evaluating sphincter function and in biofeedback training. Defecography involves imaging the rectum after filling it with contrast material, and then observing the process, rate, and completeness of rectal evacuation using fluoroscopy. Its usefulness in the evaluation of fecal incontinence is limited to cases of rectal prolapse and for the diagnosis of rectocele and enterocele.
Pudendal nerve testing -- this test uses an electrode to measure pudendal nerve conduction time, known as pudendal nerve terminal motor latency (PNTML) -- thus allowing further investigation for nerve injury (5). Normal PNTML value is 2.2 milliseconds; a value between 2.2 and 2.6 milliseconds indicates probable nerve damage; a value of 2.6 milliseconds or greater confirms nerve damage. Clinical use of PNTML is controversial; it helps diagnose nerve injury, but is currently reserved for investigational purposes.
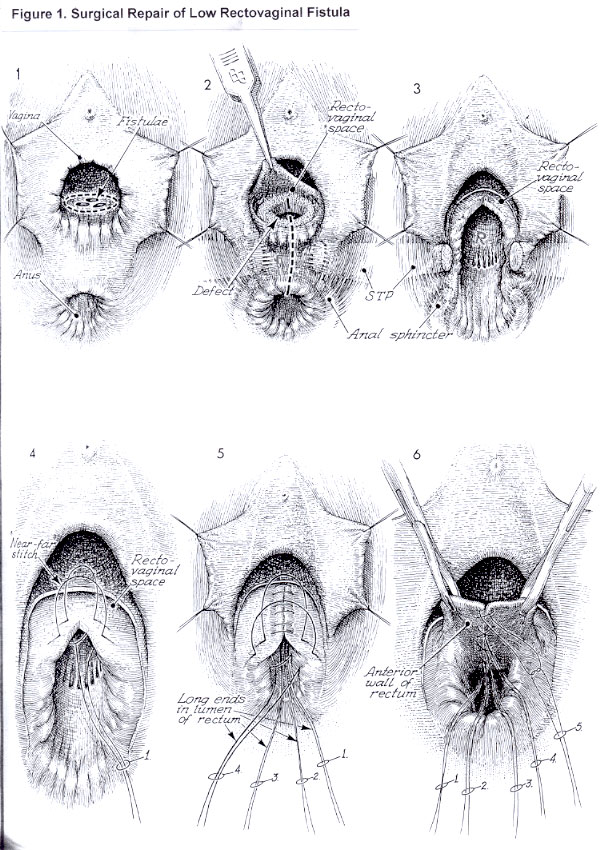
Surgical Repair of Low-Rectovaginal Fistula with Damaged Perineal Body
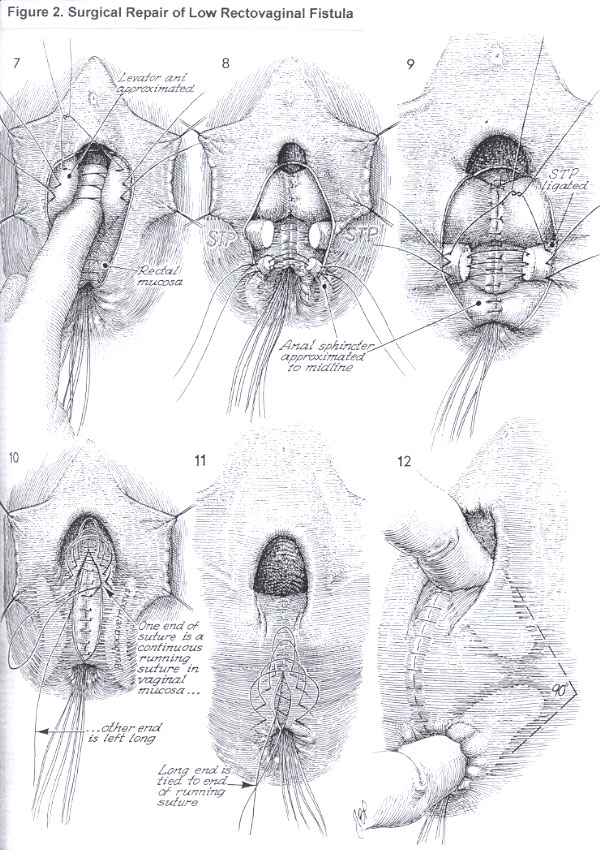
Rectovaginal fistulae may present as multiple fistulae in a so-called honeycomb appearance or as one single fistula. It is important to excise the entire fistula tract of all fistulae. Concern may exist for the competence and continuity of the transected and reconstructed anal sphincter muscle. Transaction of an otherwise competent anal sphincter and careful and proper reconstruction with suturing the fascia of the muscle should not be associated with incompetence of the sphincter and fecal incontinence secondary to that incompetent sphincter (6). An incision that encompasses the entire fistulae should be made in the posterior vaginal wall mucosa. The fistula tract has been removed down to the rectal mucosa. The margins of vagina that remain are elevated and mobilized with sharp dissection. A perineotomy incision is made through the vagina, the superficial transverse perineal, the anal sphincter, and anal mucosa. The rectum is repaired with a far-near-near-far inverting suture that inverts the mucosa into the lumen of the rectum. Care is taken that the knot is tied in the rectum to prevent the knot from becoming a wick for bacteria in this area. The rectum is repaired down to the anal mucosa; the sutures are then cut. After the rectal mucosa has been sutured, a decision must be made to bring in an exterior source of blood supply, such as the bulbocavernosus muscles with their vestibular fat pad. If that is to be performed, it should be performed at this point, and the bulbocavernosus muscle with its fat pad should be sutured over the rectal suture line before beginning the posterior repair with plication of the levator muscle in the midline. After the rectal mucosa has been sutured closed, the finger of the left hand is placed on the top of the rectal suture line. This invagination produces prominence of the levator ani muscles. Delayed synthetic absorbable suture is placed in the levator muscles to plicate them on top of the rectal suture line. The levator plication has taken place over the rectal suture line. The stumps of the superficial transverse peritonea muscle must be identified, especially with their fascia sheaths. The anal sphincter muscle should be identified, and care should be taken to identify its fascia sheath. Sutures are placed through the fascia sheath and muscle. Generally, four sutures are used in a points-of-the-compass pattern.
The vaginal mucosa is closed with a running synthetic absorbable suture. The knot is tied at the top of the vagina, and one strand of the knot is left long, coming on top of the levator repair underneath the vaginal mucosa. This strand of suture, when tied, will further plicate the top of the vagina posteriorly on top of the rectum, creating the so-called hockey-stick pattern of the vaginal canal. The suture extends out over to the skin of the perineal body. The long end is tied to the end of the running suture. When this is performed, the upper vagina is pulled posteriorly onto the rectum. A finger could be inserted in the vagina, and a finger should be inserted in the rectum. These fingers should make a 90o angle. The presence of an internal anal sphincter defect should be sought carefully at the time of primary anal sphincter repair. Disruption of the internal anal sphincter represents a more severe injury and such patients merit follow-up at a dedicated specialist clinic (7). Postoperatively, the patient is placed on running daily doses of laxatives and a low residual diet. After each bowel movement perineum should be cleaned with antiseptic solution.
Figure 1 | Figure 2
{kind=link}
{kind=link}
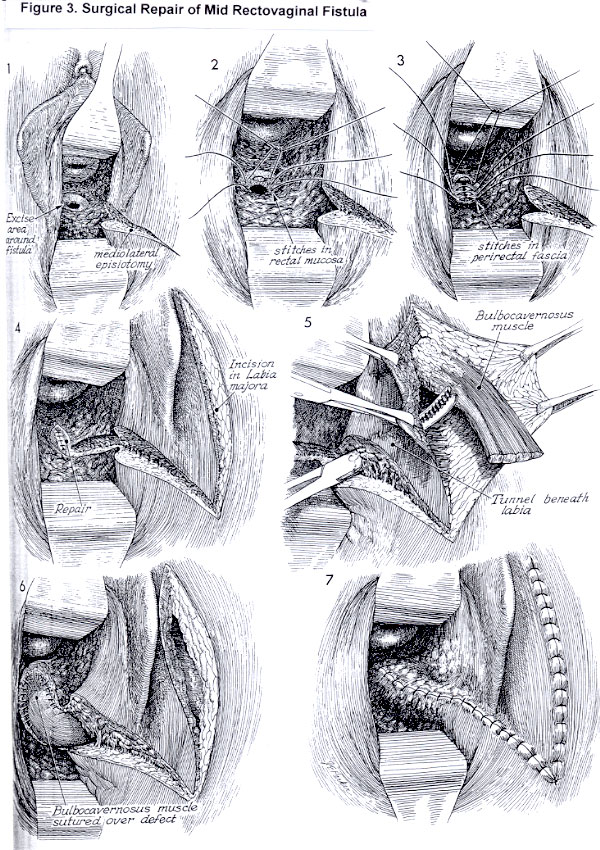
Mid-level Rectovaginal Fistula Repair
Occasionally, a fistula high inside a narrow vagina is difficult to expose. Therefore, a mediolateral episiotomy should be performed without hesitation to allow maximum exposure to the operating site. If adequate exposure cannot be obtained completely from vaginal approach, the abdominal route should be considered, particularly in those cases where the fistula is high in a deep vagina (8). Extreme care should be taken that the bowel mucosa is adequately mobilized and that devitalized, scarred, or avascular portions of the mucosa have been excised. If the intestinal mucosa cannot be mobilized and it is apparent that the closure of the intestinal mucosa will be under tension, the surgeon should perform a laparotomy and totally mobilize the rectosigmoid colon from above. Many fistula repairs fail because this is not done. After adequate mobilization of the intestinal mucosa, the edges of the intestinal mucosa are closed in an inverting fashion with interrupted 3-0 absorbable synthetic suture. The perirectal fascia and even some levator ani muscle may be drawn into a second layer of closure. If an outside blood supply is desirable, bulbocavernosus muscle is dissected and sutured over the perirectal fascia. The edges of the vaginal mucosa are then approximated with interrupted 2-0 absorbable synthetic sutures. It is highly recommended that the patient use a stool softener for 3-6 months following fistula repair.
Figure 3
{kind=link}
High Rectovaginal Fistula Repair
Most surgeons use a transabdominal approach for the repair of a high rectovaginal, or colovaginal fistula. The cause of high fistulas is usually inflammatory, including diverticulitis and Crohn's disease. Radiation injury, traumatic injury, and carcinoma almost must be considered. Bowel resection with primary reanastomosis using non-diseased tissue is the most successful approach.
Fecal Diversion
Diversion of fecal stream is sometimes required to allow adequate healing of the rectovaginal septum. Construction of stoma is rarely necessary before attempt at primary repair. However, if perineal sepsis is severe, early diversion of the fecal stream may be necessary. Diversion of the fecal stream by construction of a proximal stoma should be considered following a complex repair of rectovaginal fistula, such as a coloanal anastomosis or myofascial grafting. In addition, if previous attempts at repair of a rectovaginal fistula have failed, consideration should be given to construction of a stoma before an additional attempt at surgical reconstruction.
Managing Severe Perineal Lacerations
Anal sphincter tears resulting from vaginal delivery occur in 0.7% to 19.3% of births, mostly during a first pregnancy. The best available data do not support the liberal or routine use of episiotomy (9). Complications of anal sphincter laceration include anal incontinence, fecal urgency, perineal pain and sexual dysfunction. Five key risk factors of severe lacerations are: 1) midline episiotomy, 2) forceps of vacuum delivery (vacuum being less traumatic than forceps), 3) Asian ancestry, 4) high birth-weight, and 5) first birth. The risk of laceration during a second delivery in women who have had a previous tear is increased two to five times over women who had no history of overt laceration. Recurrence risk is highest when the second delivery is operative vaginal or when episiotomy is performed. Ultrasound assessment of the anal sphincter may be indicated in all women who are important. The general principles of treatment are to identify the underlying cause of incontinence and direct therapy based on these findings. The physician and patient must formulate a treatment plan based on the severity of the incontinence and degree of social impairment. In general, a trial of non-surgical therapy is recommended before proceeding to surgery.
Aims of non-surgical management -- are to increase anorectal sensation, and to increase the strength of the external sphincter and pelvic floor. Diet and medical therapy remains the first line of treatment given the high rate of underlying neuromuscular damage. The patient's diet should include adequate fiber and fluid intake to promote regular, soft, bulky stools. High-fiber foods including whole-wheat grains, fresh vegetables, and beans should be advised. Bulking agents like methylcellulose (eg, Citrucel), or psyllium (eg, Metamucil) can be helpful. Stool frequency can be reduced with antidiarrheal drugs like loperamide (2-4 mg 2 or 3 times daily) or diphenoxalate (eg, Lomotil). Altiflatulants are also recommended. Amitryptiline is useful in some women with idiopathic fecal incontinence (10). Biofeedback therapy, pelvic floor rehabilitation with biofeedback and/or electrical stimulation -- which focuses on the common neuromuscular etiology of fecal incontinence -- is the mainstay of non-surgical management. Some centers report a success rate as high as 70% with this therapy.
Operative therapy -- should be considered when non-surgical interventions have failed or in which distinct anatomic defects are present. Anterior overlapping external sphincteroplasty is done in patients with obstetric or iatrogenic disruption of the external anal sphincter. The success rate of sphincteroplasty ranges from 40% to 75% in appropriately selected patients. Total pelvic floor repair may help patients with neurogenic or idiopathic fecal incontinence. The principle of this procedure is to restore the anorectal angle, lengthen the anal canal, and create a circumferential buttress around the anorectum. In this rather extensive surgery, the surgeon plicates the puborectalis, ischiococcygeus, and iliococcygeus muscles to the rectum; the levator muscles and the external anal sphincter are plicated anteriorly. Success rates vary from 14% to 55%. Artificial anal sphincter procedure involves placing a cuff around the anal canal and a pressure-regulating balloon and pump in the labia majora (11).
Strategies for Managing Subsequent Pregnancies
Debate continues about elective cesarean section in women with occult sphincter injury. After sphincter laceration, or rectovaginal repair, clinicians can only determine the best delivery method for a subsequent pregnancy by discussing it with the patient. It is essential to document transient or permanent anal incontinence symptoms following the previous delivery. At the time of counseling, it is important to inform the risk of repeat laceration with another vaginal delivery. Continent women are less likely to develop anal incontinence than women who previously had symptoms of either transient or persistent anal incontinence. Nearly all women with anal incontinence will experience deterioration of their symptoms. Risks of cesarean delivery must also be discussed. Operative delivery and episiotomy should be avoided, because they compound the risk for further damage in all these women. After a thorough consultation about the risks and benefits of attempting a repeat vaginal delivery, elective cesarean delivery is appropriate for symptomatic patient (12).
Summary
The advice you give a pregnant patient who has suffered an anal sphincter laceration during a previous delivery can have a critical impact on her quality of life. With another vaginal birth, she is more likely to suffer a repeat anal sphincter tear and worsening symptoms of anal incontinence. Sexual dysfunction may also be at stake. Despite all this, there are no easy answers, because the best way to manage a subsequent pregnancy of a woman with a previous tear is controversial.
References
- Abromowitz L, Sobhani I, Ganansia R, et al. Are sphincter defects the cause of anal incontinence after vaginal delivery? Results of a prospective study. Dis Colon Rectum. 2004;43:590-596; discussion:596-598
- Vangeenderhuysen C, Prual A, et al. Obstetric Fistulae: incidence for sub-Saharan Africa. Int J Obstet Gyecol. 2001;73:65-66.
- Rafferty JF. Rectovaginal Fistula. In: Urogynecology and Reconstructive Pelvic Surgery. 2nd Edition; p. 277-283. publishers: Mosby. 1999.
- Barnett JL, Hasler WL, Camilleri M. American Gastroenterological Association medical position statement on anorectal testing techniques. American Gastroenterological Association. Gastroenterology. 1999;116:732-740.
- Sze EH, Anal incontinence among women with one versus two complete third-degree perineal lacerations. Int J Gynecol Obstet. 2005;90:213-217.
- Wheeless CR. Atlas of Pelvic Surgery. 3rd Edition. Rectovaginal Fistula Repair; p 127-131. Publishers Willams & Wilkins.
- Mahony R, Behan M, Daly L, et al. Internal anal sphincter defect influences continence outcome after obstetric anal sphincter injury. Am J Obstet Gynecol. 2007;196:217-218.
- Radman MS, Al-Suleiman SA, et al. Surgical treatment of rectovaginal fistula of obstetric origin: A review of 15 years' experience in a teaching hospital. J Obstet Gynecol. 2003;23(6):607-610.
- ACOG Practice Bulletin. Episiotomy. Clinical management guidelines for obstetricians-gynecologists. Number 17. April 2006. Obstet Gynecol. 2006;107:957-962.
- Santoro GA, Eitan BZ, Pryde A, et al. Open study of low-dose amitriptyline in the treatment of patients with idiopathic fecal incontinence. Dis Colon Rectum. 2000;43:1676-1682.
- Giamundo P, Welber A, Weiss EG, et al. The Procon incontinence device: a new non-surgical approach to preventing episodes of fecal incontinence. Am J Gastroenterol. 2002;97:232-236.
- McKenna DS, Ester JB, Fischer JR, et al. Elective cesarean delivery for women with a previous anal sphincter rupture. Am J Obstet Gynecol. 2003;189:1251-1259.
Published: 23 July 2009
Dedicated to Women's and Children's Well-being and Health Care Worldwide
www.womenshealthsection.com