


Managing Vesico-vaginal Fistula
Neeraj Kohli, MD, MBA
Division of Urogynecology and Reconstructive Pelvic Surgery
Brigham and Women's Hospital
Assistant Professor, Dept. of Ob/Gyn
Harvard Medical School
Boston, Massachusetts
and
John R. Miklos, MD
Atlanta Urogynecology Associates
Northside Hospital
Assistant Professor, Department of Ob/Gyn
Medical College of Georgia
Atlanta, Georgia
Introduction
First reported by Derry in 1935 upon examination of the mummified remains of Egyptian Queen Henhenit (11th Dynasty, 2050 BC), the vesico-vaginal fistula (VVF) continues to remain a challenging condition for the gynecologic surgeon. Of the various uro-genital fistulas previously described, the vesico-vaginal fistula (VVF) is the most common due to its relationship to various obstetric and gynecologic risk factors. However, presentation and prognosis can be variable depending on the location, size, and coexisting factors associated with fistula formation. Fortunately, the diagnosis and surgical management of vesico-vaginal fistulas is associated with high cure rates if performed by trained gynecologic surgeons.
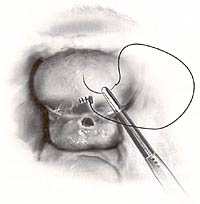
Vesicovaginal fistula |
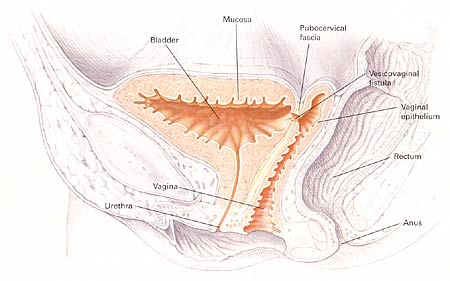 |
Pelvic cross section depicting high vescovaginal fistula. |
Risk Factors
Although the exact incidence of vesico-vaginal fistula in the United States is unknown, estimates range between 0.01 to 0.04% of gynecologic procedures. In developing countries vesico-vaginal fistulas are more common and are related to obstructed labor due to unattended deliveries, small pelvic dimensions, malpresentation, poor uterine contractions and introital stenosis. The primary cause of vesico-vaginal fistula in the United States is related to gynecologic surgery. In a series of 303 women with genitourinary fistula by Lee et al., fistulas were related to gynecologic surgery in 82%, obstetric events in 8%, radiation therapy in 6%, and trauma or fulguration in 4%. (1) Rare causes of VVF include lymphogranuloma venereum, tuberculosis, syphilis, bladder stones, retained foreign body in the vagina, and trauma. Spontaneous vesico-uterine fistula has also been reported as a rare complication following uncomplicated vaginal birth after Caesarean section. (2) Most commonly, vesico-vaginal fistulas in developing countries are associated with benign gynecologic surgery, especially hysterectomy, and are caused by extensive dissection between the bladder and the uterus, unrecognized bladder laceration, inappropriate stitch placement, and/or devascularization injury to the tissue planes. Concurrent ureteric involvement has been reported to be as high 10-15% of vesico-vaginal fistula cases. Patient risk factors which may predispose to development of vesico-vaginal fistula include prior pelvic surgery, history of PID, pelvic malignancy, endometriosis, infection, diabetes, and anatomic distortion. The presence of these risk factors should be considered pre-operatively and patients counseled accordingly.
Classification
Proper classification of a vesico-vaginal fistula can aid the gynecologic surgeon in planning the appropriate surgical treatment. Obstetric vesico-vaginal fistulas may be classified depending on their location, cause, complexity, or site of obstruction. Gynecologic fistula is classified as simple or complicated and may have important implications for surgical approach as well as prognosis for cure. (3) Although the simple vesico-vaginal fistulas are usually uncomplicated surgical cases with good prognosis, complicated vesico-vaginal fistulas are challenging even for the most experienced and skilled gynecologic surgeon.
Classification of vesicovaginal fistulae |
|
Classification |
Description |
Simple |
|
Complicated |
|
Source: OBG MANAGEMENT. August 2003 |
|
Diagnosis
The diagnosis of vesico-vaginal fistula begins with high clinical suspicion based on patient symptomatology. Patients will typically present at variable time intervals after the antecedent event (childbirth, pelvic surgery, radiation therapy, etc.) with primary complaints of constant painless urinary incontinence. Some patients will report exacerbation during physical activities which can sometimes lead to the erroneous diagnosis of uncomplicated stress incontinence. If the fistula is small, intermittent leakage with increased bladder distention or physical activity may be noted. Other patients may complain of vaginal discharge or hematuria. If there is concurrent ureteric involvement, the patient may experience constitutional symptoms including fever, chills, flank pain, or gastrointestinal symptoms. Timing of the presentation is variable. If related to traumatic childbirth, most patients experience urine leakage within the first 24-48 hours. Following pelvic surgery, symptoms will usually present within the first 30 days after surgery. In contrast, radiation induced fistulas have a slow development process secondary to slowly progressive devascularization necrosis and may present between 30 days and 30 years following the antecedent event. High clinical suspension is the key to prompt and accurate diagnosis of vesico-vaginal fistula.
On physical exam: Pooling of fluid in the vagina may be noted and should be sent for analysis if the diagnosis is unclear. A careful speculum exam allowing visualization of the entire anterior vaginal wall should be performed to identify the fistula tract. In many cases, the fistula is grossly visible. The location of the fistula in relation to the vaginal apex and bladder trigone should be inspected and the quality of the surrounding tissue (inflammation, edema, or infection) noted. In some cases of small fistula, no obvious tract may be noted. Bimanual exam with careful palpation of the anterior mall may help isolate the location with palpation of a surrounding zone of induration. If no fistula is noted despite high clinical suspicion, a simple dye filling test of the bladder can be performed in the office. The bladder is filled with a dyed fluid (normal saline with indigo carmine) using a urinary catheter, and repeat pelvic exam with a half speculum is performed to visualize the anterior wall. The patient is asked to cough and bear down and the location of the fistula is confirmed with visualization of urine leakage. If this test is negative, a tampon is inserted and the patient is asked to perform 10-15 minutes of provocative maneuvers including stair climbing and jumping in place. The tampon is removed and visualization of dye beyond the most distal edge of the tampon confirms the presence of a fistula. A variation of this technique is the double dye test where the patient is given oral phenazopyridine (Pyridium), the bladder is filled, and a tampon inserted. The presence of blue staining (Indigo Carmine) suggests vesico-vaginal or urethra-vaginal fistula while red staining (Pyridium) suggests uretero-vaginal fistula.
Diagnostic Testing is helpful in ruling out concurrent pathology and formulating an appropriate treatment plan. Routine testing should include a urinalysis and culture to rule out coexisting urinary tract infection, electrolyte panel to evaluate renal function, and complete blood cell count to rule out systemic infection. Cystoscopy should be performed to visualize the fistulous tract, assess location of the fistula in relation to the ureters and trigone, assure bilateral ureteral patency, and exclude foreign body or suture placement in the bladder. In patients with a history of uro-genital malignancy, a biopsy of the fistula tract and urine cytology is warranted. Radiologic studies are recommended prior to surgical repair of a vesico-vaginal fistula to fully assess the fistula and exclude the presence of multiple fistulas. An intravenous pyelogram is recommended to exclude concurrent uretero-vaginal fistula or ureteral obstruction. A targeted fistulogram may be indicated if conservative therapy including expectant management, continuous bladder drainage, fulguration, or fibrin occlusion therapy is to be recommended.
Treatment
Symptomatic vesico-vaginal fistula merits appropriate treatment as spontaneous closure is uncommon. Appropriate treatment will depend on various factors including size and location of the fistula, timing from the antecedent event, and severity of symptoms, quality of surrounding tissue, and clinician experience and surgical skills.
Conservative Management
A small number of fistulas may heal following prolonged bladder drainage thru a transurethral or suprapubic catheter if diagnosed within the first few days of surgery. Zimmern has recommended a conservative approach to small fistulas if the patient's complaints of urinary incontinence are resolved with insertion of a Foley catheter. In this case, bladder drainage is continued for three weeks and the fistula is then reevaluated. If the fistula has diminished in size, a trial of continued catheter drainage for an additional three weeks is beneficial with a high rate as spontaneous closure. If there is no change, the fistula is unlikely to resolve spontaneously. (4) Most authors report variable success ranging from 2-80% with treatment of vesico-vaginal fistula using chronic bladder drainage, and there is increased chance of success if the fistula is diagnosed within seven days of index surgery, is less than 1 cm in size, is simple without associated carcinoma or radiation, and is subject to at least four weeks of constant bladder drainage. Persistent, large, or complex fistulas are best treated with surgical intervention.
Surgical Management
Although the basic principles of fistula closure (mobilization of tissue, good vascular supply, and non-opposing tissue lines) remain the same, there have been several recent advances in the treatment of vesico-vaginal fistula with respect to timing of repair and surgical technique. General principles of surgical repair of vesico-vaginal fistula include adequate exposure, good hemostasis, wide mobilization of the bladder and vagina, resection of devascularized tissue and removal of foreign body, tension free closure, non-opposition of suture lines, and confirmation of a water tight seal on bladder closure, and postoperative bladder drainage for 10-14 days.
Timing of the fistula repair has been controversial and this can be a difficult dilemma for the physician and patient alike. Traditionally, an interval of 3 months has been recommended between the fistula repair and index surgery and up to 1 year in cases of radiation induced fistula. There is little data to support these recommendation and most experts currently recommended an individualized approach to each patient, delaying the surgery until surrounding tissue inflammation and infection have resolved or been treated. Use of estrogen, antibiotic, and/or steroids to facilitate healing during this period has been recommended. (5) Several authors have reported comparable success with early and late surgical repair of surgery induced fistulas based on these principles. (6) (7) (8)
Vaginal Approach:
Most vesico-vaginal fistulas can be surgically corrected using a vaginal approach. Traditionally, a Latzko partial colpocliesis or fistulectomy with flap splitting closure have been advocated. There is a continued debate whether resection of the fistulous tract is necessary. Advocates of the conservative approach feel that wide resection of the tract increases the size of the fistula and subsequent risk of recurrence. In addition, the surrounding fibrous tissue may reinforce the fistula repair. Proponents of fistulectomy counter that resection of the fistula and exposure of healthy tissue optimizes wound healing and improves surgical success rates. Various authors have reported equally high success rates would both techniques. (9) (10)
The Latzko partial colpocliesis, first reported in 1942, (11) continues to be a commonly performed vaginal procedure for the treatment of vesico-vaginal fistulas associated with success rates of 90-100%. Advantages of this procedure include short operative time, low inter- and postoperative morbidity, and low risk of ureteral injury. After identification of the fistulous tract, a circumferential incision is made in the vagina approximately 2 cm from the fistulous tract. The vagina is mobilized and then closed over the fistulous tract with delayed absorbable suture in double layer without disturbing the bladder mucosa. The vaginal mucosa is then closed, completing the repair.
Alternatively fistulectomy with a flap splitting closure begins with resection of the fistulous tract to expose healthy tissue at the wound margins. The defect is then closed in a multilayer fashion beginning with the bladder mucosa, bladder serosa, pubo-cervical fascia, and vaginal mucosa. Care should be taken to avoid tension on suture lines and a fascial flap is created to prevent opposition of the incision planes and reduce risk of recurrence. Cystoscopy should be done prior to and following the procedure to exclude ureteral compromise. In cases with high risk of recurrence such as complex or large fistula, a Martius fat pad graft should be interposed between the layered closure to promote vascularization and reduce risk of recurrence. (12) Placement of a cadaveric biomaterial graft has also been reported, reducing the need for complicated flap procedures. (13)
Vesicovaginal Fistula Repair | |
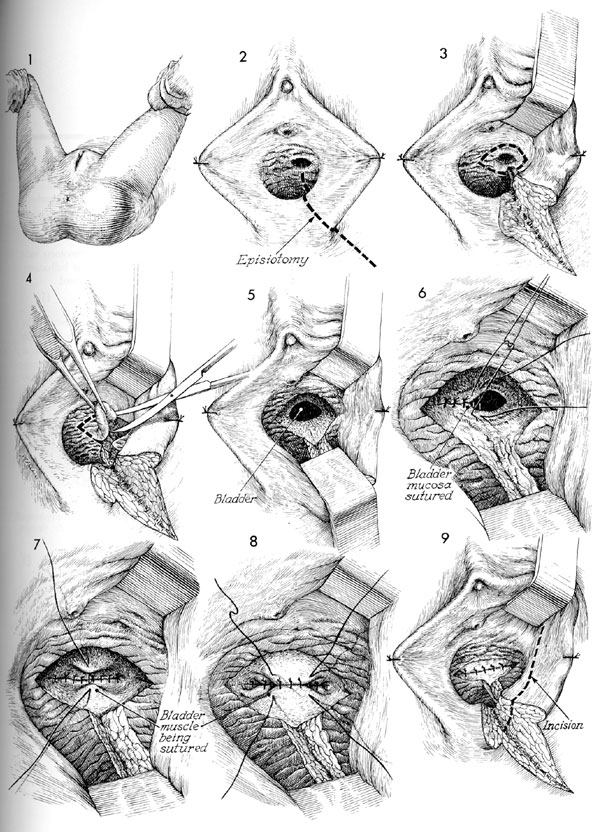 | 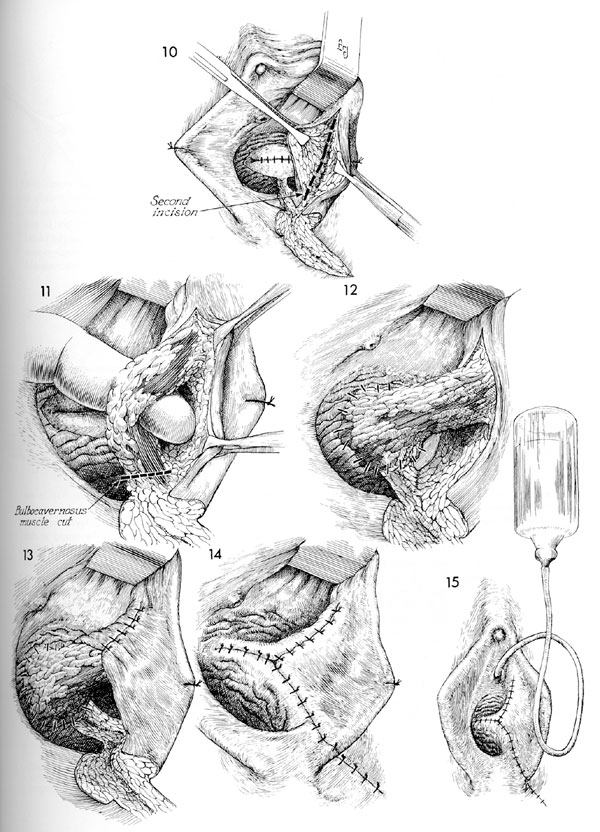 |
Click to view detail. Source: Atlas of Pelvic Surgery, third edition | |
Abdominal/Laparoscopic Approach:
Although most vesico-vaginal fistulas can be surgically corrected via the vaginal approach, the abdominal route may be preferred for high and inaccessible fistulas, large complex fistulas, multiple fistulas, concurrent uterine or bowel involvement, or need for ureteral reimplantation. The abdominal approach may be facilitated by cystoscopically guided placement of a catheter thru the fistulous tract to assist in subsequent identification and dissection. A vertical skin incision is recommended to optimize visualization and allow mobilization of an omental flap if needed. The bladder is exposed and a high extraperitoneal cystotomy is intentionally created to visualize the fistulous tract. Ureteral stents should be placed if the fistula is in close proximity to the ureteral orifice. The bladder incision is extended to the fistulous tract which is then completely excised following mobilization of the vagina. The vagina and bladder are then closed with interrupted delayed absorbable suture in a double layer fashion. Transposition of an omental flap between the vaginal and bladder incisions is recommended to promote vascularization, minimize opposition of suture lines, and reduce risk of recurrence.
Abdominal Repair |
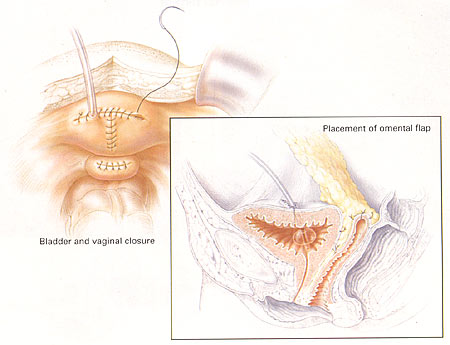 |
| Abdominal repair of vesicovaginal fistula, with closure of bladder defect and posterior cystotomy and separate closure of vaginal defect. Note the omental flap pictured in the insert. Source: OBG MANAGEMENT. August 2003 |
A similar repair has been reported laparoscopically with equally good results, but requires advanced laparoscopic skills with endoscopic suturing and knot tying. (14)
Laparoscopic Repair |
 |
| Laparoscopic repair of vesicovaginal fistula. Source: OBG MANAGEMENT. August 2003 |
Suggested Guidelines:
- Conservative therapy should be reserved for simple fistulae that are less than 1 cm in size, diagnosed within 7 days of the index injury, lacking associated carcinoma or radiation, and subject to at least 4 weeks of constant bladder drainage.
- Surgical risk factors include prior pelvic surgery, history of pelvic inflammatory disease, pelvic malignancy, endometriosis, infection, diabetes, and anatomic distortion.
- In surgical repair, the Latzko partial colpocleisis or fistulectomy with flap-splitting closure is preferred.
Conclusion
Despite a long clinical history and extensive surgical experience, vesico-vaginal fistula continues to challenge even the most experienced gynecologic surgeon. The key is prevention with good surgical technique and identification and repair of the bladder injury at the time of index surgery. Patients with characteristics symptoms following an antecedent event should be treated with high clinical suspicion. Physical exam, laboratory evaluation, and ancillary testing should make the correct diagnosis in virtually all patients. If small and treated immediately after the antecedent event, conservative therapy with prolonged bladder drainage may be effective. However, most patients will require surgery, which can usually be performed successfully through a vaginal route. Abdominal procedures are reserved for more complicated cases. Adherence to strict surgical principles for fistula repair will result in optimal cure rates with minimal complications. Using these guidelines, both the clinician and patient should feel comfortable with the successful management of vesico-vaginal fistula.
References:
- Lee RA, Symmonds RE, Williams TJ. Current status of genitourinary fistula. Obstet Gynecol 1998; 72: 313-315.
- Miklos JR, Sze EHM, Parobeck D, et al. Vesicouterine fistula: a rare complication of vaginal birth after Caesarean. Obstet Gynecol 1995; 86: 638-639.
- Elkins TE, Thompson JR. Lower urinary tract fistulas. Urogynecology and Reconstructive Pelvic Surgery, 2nd ed. Walters M, Karram MM, ed. Mosby Publishers 1999: 355-365.
- Zimmern PE, Hadley HR, Staskin D: Genitourinary fistulas: vaginal approach for repair of vesicovaginal fistulas. Clin Obstet Gynaecol 1985; 12(2): 403-13
- Margolis T, Mercer LJ: Vesicovaginal fistula. Obstet Gynecol Surv 1994 Dec; 49(12): 840-7
- Blaivas JG, Heritz DM, Romanzi LJ: Early versus late repair of vesicovaginal fistulas: vaginal and abdominal approaches. J Urol 1995 Apr; 153(4): 1110-2.
- Blandy JP, Badenoch DF, Fowler CG: Early repair of iatrogenic injury to the ureter or bladder after gynecological surgery. J Urol 1991 Sep; 146(3): 761-5.
- Cruikshank SH: Early closure of posthysterectomy vesicovaginal fistulas. South Med J 1988 Dec; 81(12): 1525-8.
- Raz S, Bregg KJ, Nitti VW: Transvaginal repair of vesicovaginal fistula using a peritoneal flap. J Urol 1993 Jul; 150(1): 56-9
- Iselin CE, Aslan P, Webster GD: Transvaginal repair of vesicovaginal fistulas after hysterectomy by vaginal cuff excision. J Urol 1998 Sep; 160(3 Pt 1): 728-30.
- Latzko W: Postoperative vesicovaginal fistulas: genesis and therapy. Am J Surg 1942; 58: 211-8.
- Punekar SV, Buch DN, Soni AB: Martius' labial fat pad interposition and its modification in complex lower urinary fistulae. J Postgrad Med 1999 Jul-Sep; 45(3): 69-73
- Miklos JR, Kohli N. Rectovaginal fistula repair utilizing a cadaveric dermal allograft. Int Urogynecol J Pelvic Floor Dysfunct. 1999;10(6):405-6.
- Nezhat CH, Nezhat F, Nezhat C: Laparoscopic repair of a vesicovaginal fistula: a case report. Obstet Gynecol 1994 May; 83(5 Pt 2): 899-901
Dedicated to Women's and Children's Well-being and Health Care Worldwide
www.womenshealthsection.com