新生儿B组链球菌感染WHEC实践公报和临床管理准则的医疗保健提供商。教育补助金所提供妇女保健和教育中心( WHEC ) 。 Group B streptococcal (GBS) infection remains the most common cause of neonatal early-onset sepsis and a significant cause of late-onset sepsis among young infants. Administration of intrapartum antibiotic prophylaxis is the only currently available effective strategy for the prevention of perinatal GBS early-onset-disease, and there is no effective approach for the prevention of late-onset disease. The Women's Health and Education Center (WHEC) reaffirms the use of universal antenatal microbiologic-based testing for the detection of maternal GBS colonization to facilitate appropriate administration of intrapartum antibiotic prophylaxis. The purpose of this document is to provide healthcare providers, with updated information regarding the epidemiology of GBS disease, as well current recommendations for the evaluation of newborn infants at risk for GBS disease, and for treatment of those with confirmed GBS infection. This review addresses the epidemiology, microbiology, disease pathogenesis, and management strategies for neonatal early- and late-onset GBS infection. Maternal management is discussed in the "Prevention of Group B Streptococcal Infections in Newborn." IncidenceHealthcare providers should recognize that GBS early-onset-disease can occur among term infants born to mothers who have screened negative for GBS. Authors of one single-center study with policies mandating universal screening-based GBS intrapartum antibiotic prophylaxis found that over an 8-year period, 17 GBS early-onset cases occurred among term infants and 14 of 17 (82.4%) of the mothers has screened negative for GBS (1). Multistate Active Bacterial Core surveillance's (ABC's) data in 2003-2004 identified 189 cases of GBS early-onset-disease among term infants and determined that 116 of 189 (61.4%) occurred among infants born to women who screened negative for GBS (2). GBS early-onset disease may occur in infants of mothers who screened negative for GBS because of changes in maternal colonization status during the interval from screening to presentation for delivery or because of an incorrect technique in obtaining vaginal-rectal screening cultures or in laboratory processing. Prevention of Group B Streptococcal Infections in Newborns; Antepartum and Intrapartum ManagementCurrent Epidemiology of Neonatal GBS InfectionEarly-Onset GBS Infection Newborn infants readmitted to the hospital within the first week after hospital discharge with culture-confirmed infection attributable to any bacteria, in this study, was approximately 5 cases per 100,000 live birth (7). Globally, outside the United States, an estimated 200,000 GBS cases of GBS early-onset-disease occurred in 2015. Stillbirth, GBS early-onset-disease, and late-onset GBS cases combined contribute to an estimated 150,000 fetal and neonatal deaths throughout the world, with the largest concentration of GBS perinatal deaths occurring in Africa (8). Late-Onset GBS Disease GBS were isolated from CSF in 20.7% of cases, and meningitis was diagnosed in 31.4% of cases. Cultures of bone and joint and peritoneal fluid yielded GBS in 1.8% of cases (10). CSF culture-positive GBS late-onset-disease occurred in the absence of bacteremia in approximately 20% of late-onset meningitis cases (incidence: 1.9 cases per 100,000 live births). Infants born at <37 weeks' gestation approximately 42% of all GBS late-onset-disease cases, and death attributable to GBS late-onset-disease occurs in preterm infants at roughly twice the rate of term infants (7.8% vs 3.4%, respectively) (10). GBS late-onset-disease complicated by meningitis has a higher patient fatality rate than with other syndromes. Pathogenesis and Risk FactorsGBS Virulence Surveillance data in the United States for invasive strains from 2006 to 2015 revealed that 93.1% of GBS early-onset-disease cases were attributable to serotypes Ia (27.3%), III (27.3%), II (15.6%), V (14.2%), and Ib (8.8%); the proportion attributable to emerging serotype IV ranged from 3.4% to 11.3% over the study period (4). Serotype III accounted for approximately 56.2% of 1,387 GBS late-onset-disease cases during 2006 to 2015, with serotypes Ia (20%), V (8.3%), IV (6.2%), and Ib (6.1%) making up most of the remaining serotypes. The capsular polysaccharide of all GBS serotypes resists complement deposition and inhibits opsonophagocytosis. Maternally derived, serotype-specific antibody to maternal colonizing GBS isolates is protective against newborn infection (12). GBS express multiple additional virulence factors, including surface proteins such as the α and β C-proteins that promote adherence and immune evasion, pore-forming toxins such as β-hemolysin and CAMP factor, and secreted proteases such as the C5a peptidase that cleaves complement. Strains vary in their expression of virulence factors, many of which are highly regulated by 2-component regulatory systems. The hypervirulent serotype III multi-locus sequence type 17 (ST17), for example, is commonly found in cases of GBS meningitis (13). Risk Assessment of Early-Onset GBS InfectionBecause the pathogenesis of GBS early-onset-disease begins with vertical transmission of GBS from mother to fetus and newborn infant, the strongest predictor of GBS early-onset-disease is maternal GBS early-onset-disease, such as the virulence of maternal colonizing isolate and the presence of maternal serotype-specific protective antibody, cannot be known to the physician at the time of neonatal risk assessment. The newborn infant's condition at birth and evolving condition over the first 12 to 24 hours after birth are strong predictors of early-onset infection attributable to any pathogen (14). In summary, at this time, evidence supports the following:
Management StrategiesThere are three Current Approaches to Risk Assessment among infants born at >35 Weeks' Gestation 1. Categorical Risk Assessment: It uses risk factor threshold values to identify infants at increased risk of GBS early-onset-disease (10). See figure 1 A below. 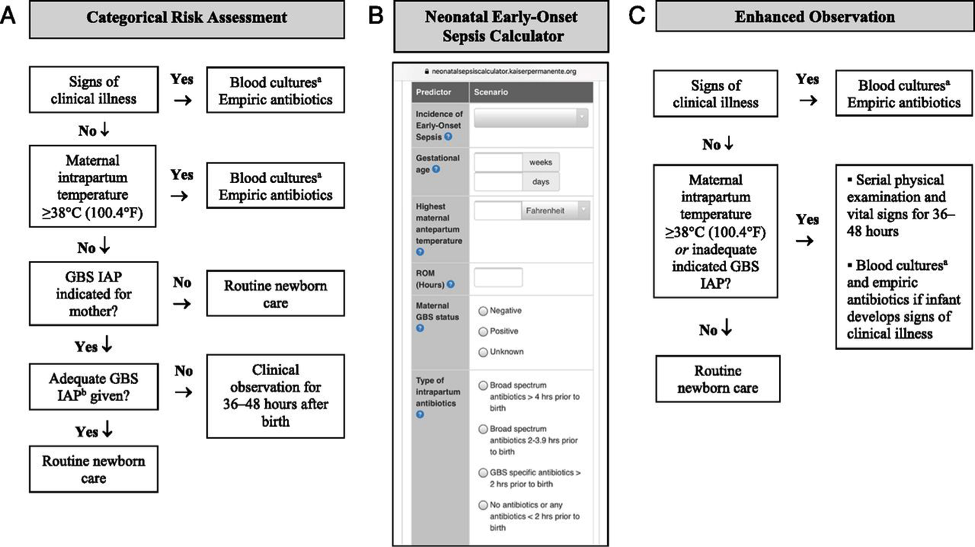 The administration of penicillin G, ampicillin, or cefazolin >4 hours before delivery is considered adequate GBS intrapartum antibiotic prophylaxis; other antibiotics or other durations of treatment <4 hours are considered inadequate when using this approach. Substantial data have been reported on the impact of using categorical risk factors to manage the risk of GBS early-onset-disease (16). However, the risk is highly variable among the newborn infants recommended to receive empirical treatment in this approach, ranging from slightly lower than the baseline population risk to significantly higher, depending on the gestational age, duration of rupture of membranes, and timing and content of administrated intrapartum antibiotics. Consequently, a limitation of this approach is that categorical management will result in empirical treatment of many relatively low-risk newborn infants. 2. Multivariate risk assessment (the Neonatal Early-Onset Sepsis Calculator): It integrates the individual infant's combination of risk factors and the newborn infant's clinical condition to estimate an individual infant's risk of early-onset sepsis, including GBS early-onset-disease. Predictive models based on gestational age at birth, highest maternal intrapartum temperature, maternal GBS colonization status, duration of rupture of membranes, and type and duration of intrapartum antibiotic therapies have been developed and validated. These models are available as a Web-based Neonatal Early-Onset Sepsis Calculator (See figure 1B above) or available @: https://neonatalsepsiscalculator.kaiserpermanente.org/ When using models, only penicillin, ampicillin, or cefazolin should be considered as "GBS-specific antibiotics." The administration of clindamycin or vancomycin alone for intrapartum antibiotic prophylaxis for any duration is currently recommended to be entered as "no antibiotics." Because the models were developed to predict risk of all bacterial causes of early-onset sepsis (and not just GBS early-onset-disease), and because these models account for other antibiotic types and indications for intrapartum antibiotic administration, "GBS specific antibiotics >2 hours prior to birth" is 1 of calculator variables. The 2-hour timing is used because multiple factors in addition to GBS intrapartum prophylaxis are considered when using the multivariate models in the Neonatal Early-Onset Sepsis Calculator. Used in this manner, threshold risk estimates prompting enhanced clinical observation or blood culture and empirical antibiotic therapy have been prospectively validated in large newborn cohorts (17). 3. Risk assessment based on newborn clinical condition: A final approach to GBS early-onset-disease risk assessment is to rely on clinical signs of illness to identify infants who may be at increased risk of infection. Among term infants, good clinical condition at birth is associated with an approximately 60% to 70% reduction in risk for early-onset infection (14). Under this approach, infants who appear ill at birth and whose who develop signs of illness over the first 48 hours after birth are treated empirically with antibiotics (18). Physicians and families must understand that the identification of initially well-appearing infants who develop clinical illness is not failure of care, but rather an anticipation outcome of this approach to GBS early-onset-disease risk management. Infants Born at <34 Weeks' Gestation, The Optimal Approach to Risk AssessmentClinician may adopt one of the following strategies to develop institutional approaches best suited to their local resources and structure of care. 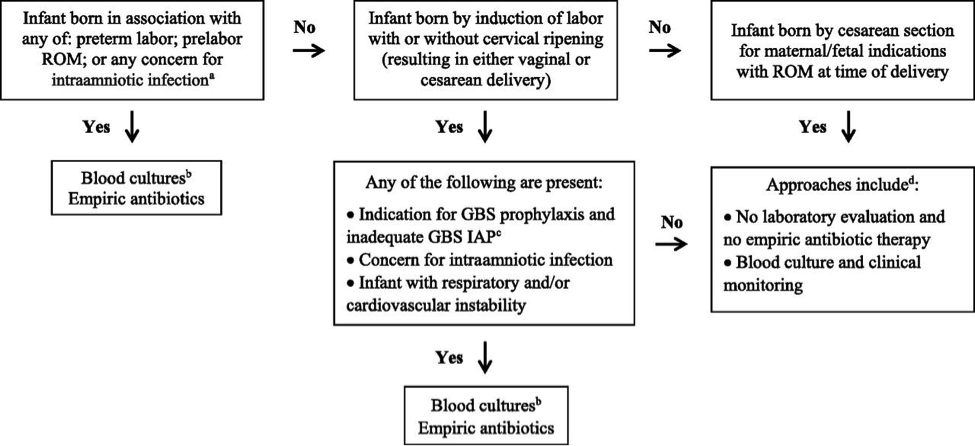 Preterm infants at highest risk for early-onset sepsis: Infants born preterm because of cervical insufficiency, preterm labor, prelabor premature rupture of membranes, intraamniotic infection, and/or acute or otherwise unexplained onset of non-reassuring fetal status are at the highest risk of early-onset sepsis and GBS early-onset-disease. The administration of GBS intrapartum antibiotic prophylaxis may decrease the risk of infection among these infants, but the most reasonable approach to these infants is to obtain a blood culture and start empirical antibiotic treatment. A lumbar puncture for culture and analysis of CSF should be considered in clinically ill infants when there is a high suspicion for GBS early-onset-disease unless the procedure will compromise the neonate's clinical condition. Preterm infants at lower risk for early-onset sepsis: Preterm infants at lowest risk for all early-onset sepsis and for GBS early-onset-disease are those born under circumstances that include all of these criteria (19):
Acceptable initial approaches of these infants include no laboratory evaluation and no empirical antibiotic therapy or blood culture and clinical monitoring. For infants who do not improve after initial stabilization and/or those who have severe systemic instability, the administration of empirical antibiotics may be reasonable but is not mandatory. Infants delivered for maternal and/or fetal indications but who are ultimately born by vaginal or cesarean delivery after efforts to induce labor and/or with rupture of membranes before delivery are subject to factors associated with the pathogenesis of GBS early-onset-disease. If the mother has an indication for GBS intrapartum antibiotic prophylaxis and adequate intrapartum antibiotic prophylaxis (penicillin, ampicillin, or cefazolin >4hours before delivery) is not given or if any other concern of infection arises during the process of delivery, the infant should be managed as recommended above for preterm infants at higher risk for GBS early-onset-disease. Otherwise, an acceptable approach to these infants is close observation for those infants who are well appearing at birth and to obtain a blood culture and to initiate antibiotic therapy for infants with respiratory and/or cardiovascular instability after birth. Clinical PresentationThe initial signs of sepsis may be subtle, and may include temperature instability, tachycardia, poor peripheral perfusion and respiratory distress. Because the progression of invasive disease is very rapid, any infant with clinical signs suggestive of infection should be treated immediately following a prompt full diagnostic evaluation; delay between presentation and therapy increases the risk of a poor outcome (20). There is no clear distinction in the clinical signs present when the infant has GBS sepsis compared with any other invasive organism. Neither the maternal screening history nor intrapartum exposure to antibiotics should affect the approach to the management of the infant with clinical signs of sepsis. Therefore, prospective therapy, while waiting culture results, should cover the most common bacteria: GBS, other streptococci, Escherichia coli, other Gram-negative organisms and Listeria monocytogenes. An infant with signs of sepsis does not require confirmatory tests other than obtaining cultures before commencing therapy, because no other tests have an adequately high negative predictive value to avoid therapy. In particular, a normal white blood count (WBC) or differential should not prevent treatment in such an infant because the negative likelihood ratio of a normal complete blood count (CBC) is approximately 0.7 (21). Limited diagnostic evaluation: It consists of CBC, and observation of vital signs every 4 hours for a period of 24 hours. The newborn can be cared for and observed in the mother's postpartum room. If the CBC shows a low total WBC of less than 5.0X109/L, then the risk of sepsis is substantially increased and a full diagnostic evaluation an initiation of therapy would usually be indicated. Full diagnostic evaluation: It consists of a CBC, blood culture and lumbar puncture (LP); a chest x-ray should be obtained if respiratory difficulties are present. LP can be deferred in unstable infants and performed later to ascertain the presence of hypoglycorrhachia or pleocytosis. Infants whose only sign of sepsis is respiratory distress may also be considered for deferment of LP if close follow-up can be ensured. Empirical and Definitive TreatmentTable 1 below shows the current recommended intravenous (IV) antibiotic regimens for confirmed early- and late-onset GBS bacteremia and meningitis (5,22). 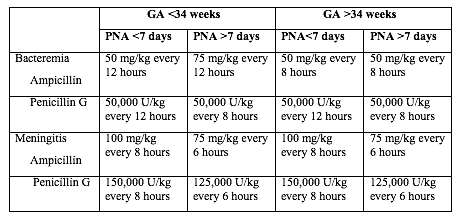 The length of antibiotic treatment is generally 10 days for bacteremia without focus and 14 days for uncomplicated meningitis; antibiotic should be given IV for the entire course. Longer therapy is used when there is a prolonged or complicated course. Some experts recommend a second LP for CSF culture 24 to 48 hours after the start of antibiotics. Additional LP and intracranial imaging are advised if there is not resolution of CSF infection, if neurologic abnormalities persist, or if focal deficits develop. Osteoarticular infection should be treated for 3 to 4 weeks and ventriculitis should be treated for at least 4 weeks. Consultation with a pediatric infectious disease specialist should be considered for meningitis and for cases with site-specific infection. Audiology testing and ongoing audiologic monitoring, if indicated, should be arranged before discharge. Recurrent GBS Disease: Recurrent neonatal and young infant GBS disease can occur after completed appropriate treatment of the primary infection (23). In this study, during 2011 to 2015 the recurrence rate was 2.8% of cases of neonatal GBS infection (24). Recurrent cases were identified 3 to 54 days after completion of the therapy for the first course. Recurrent cases are generally caused by the same GBS serotype that caused the primary infection, and persistent mucosal colonization and poor neonatal antibody responses to the first infection likely contribute to the pathogenesis or recurrent infection. it is not preventable by extension of recommended antibiotic courses nor by the addition of rifampin to eradicate mucosal colonization (25). 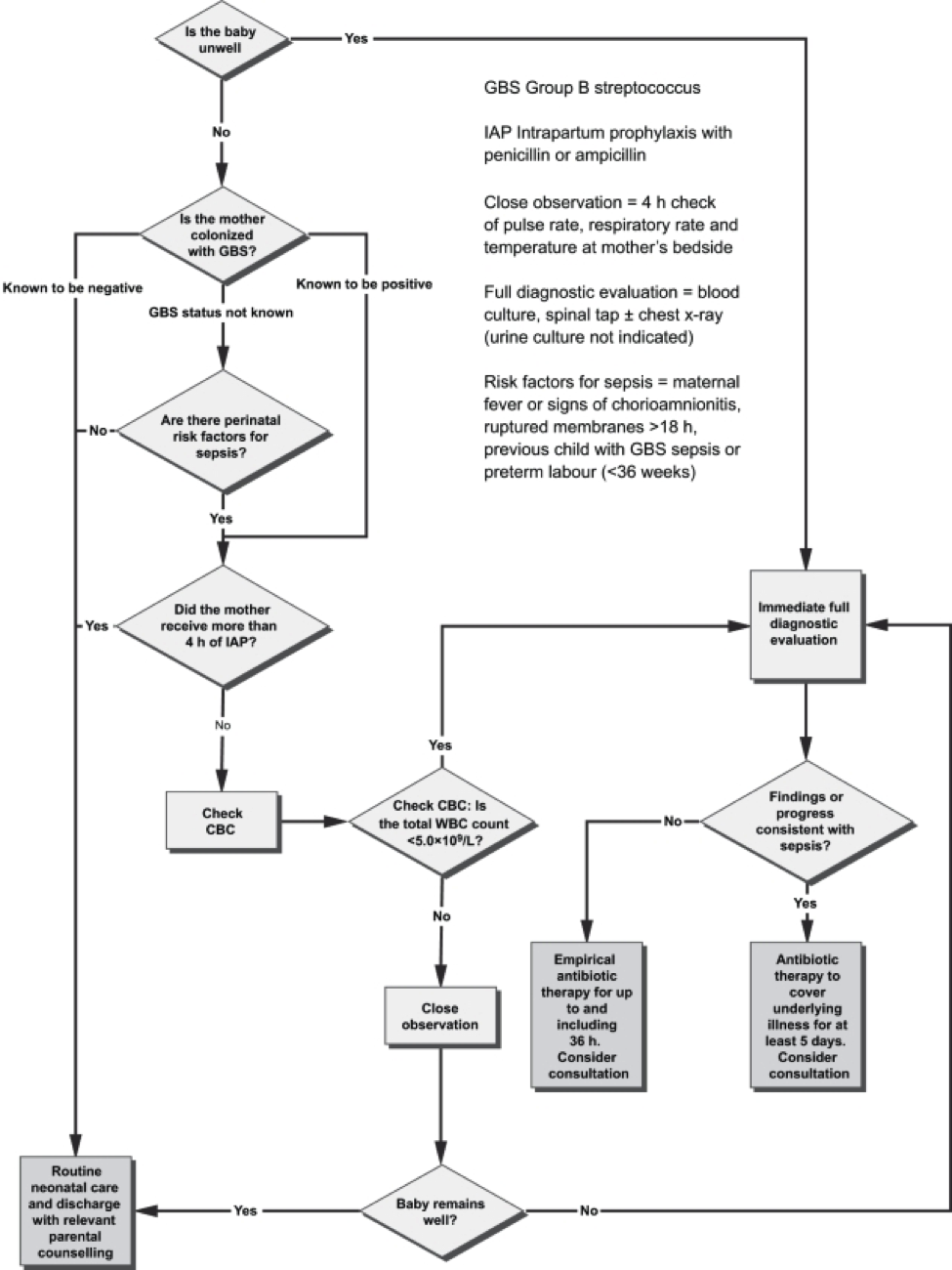 The mother who delivers at less than 37 weeks will often not have results of antenatal GBS screening available. In such a case, the infants has a 'risk factor' (prematurity) for invasive GBS disease, and if baby appear well, should have a limited diagnostic evaluation. Infants of this gestational age should not be discharged before 48 hours at the earliest. See Figure 3 above. Empirical Therapy for Infants with Positive Cerebrospinal Fluid (CSF)There are no good prospective studies to indicate optimal choice of therapy in newborn infant with possible sepsis, but ampicillin and gentamycin are usually appropriate based on the usual susceptibilities of the predominant organisms causing early-onset sepsis (21). Infants with a positive CSF evaluation or with clinical signs of meningitis if the lumbar puncture (LP) has been deferred, should be treated with antibiotics which both penetrate the CSF are active against the likely organisms (See Table 2 below). If there is information from the maternal history suggesting an organism that is unlikely to respond to these antibiotics, empirical therapy should be adjusted appropriately. Blood cultures using modern automated systems are almost always positive by 48 hours (26). Therefore, if the laboratory results and clinical course do not indicate bacterial infection, therapy may be discontinued after 48 hours. 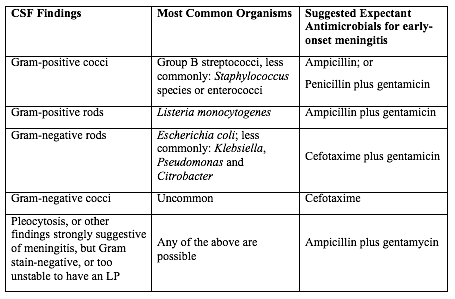 The majority of antibiotic courses are given to infants who eventually prove not to have has sepsis; strategies for further reduction of the duration of antibiotic therapy in such infants should be considered. For example, because gentamicin is usually now given once per day in the full-term infant, and ampicillin is given every 12 hours, the initial antibiotic order could be to give ampicillin for four doses every 12 hours and gentamicin for two doses every 24 hours, followed by reassessment after verification of culture results at 48 hours, and reordering the antibiotics in case of positive cultures or ongoing signs of sepsis (27). GBS Vaccine DevelopmentGBS is an important pathogen as it is the leading cause of neonatal deaths due to sepsis, meningitis or bacterial pneumonia. Although the development of an effective and safe GBS vaccine is on the agenda of many research labs, there is no GBS vaccine on the market yet. An effective vaccine is likely to prevent the majority of infant disease (both early and late onset), to avoid the limitations of intrapartum antibiotic prophylaxis and to be cost effective. A number of candidates, including capsular conjugate vaccines, have the potential to be successful vaccines. Phase II human studies with capsular conjugate vaccines have been completed successfully. Issues yet to be resolved include the safety and acceptability of vaccination during pregnancy, the durability of vaccine-derived immunity and regulatory issues required for licensure (28). The World Health Organization (WHO) has identified the development of GBS vaccine for maternal immunization as a priority, based on the high unmet medical need, assessment of technical feasibility of vaccine development and the potential value of WHO involvement. In order to accelerate GBS vaccine development, the WHO has developed a vaccine development technology roadmap, to highlight priority activities for vaccine developers, researchers and funders. It has identified 'preferred Product Characteristics' which describe the vaccine characteristics that need to be considered in relation to the public health need (29). The goal is to develop a vaccine for global use that can protect against GBS related stillbirth and invasive disease in neonates and young infants by immunizing pregnant women in the second and third trimester. The target is to provide 80% protection in fetuses/neonates against the combined risk of laboratory-confirmed GBS invasive disease-causing stillbirth and neonatal death. There are a number of challenges for GBS vaccine development. An effective vaccine needs to target over 90% of the current invasive disease isolates, either overcoming the diversity of GBS capsular types, or targeting protein expression polymorphism and prevalence. The potential exists for GBS invasive disease strain evolution and capsular switching, for which long-term strain composition is required. The role of past GBS exposure and vaccines received in previous pregnancies needs to be determined. The vaccine's immunogenicity on co-administration with other recommended vaccines in pregnancy and the impact on the immune responses to infants vaccines needs to be characterized, considering both the target antigen and similar carrier proteins. The impact of the vaccine in the presence of co-infections such as HIV and malaria in the pregnant women needs to be evaluated. An adjuvant, if used, should have a well-demonstrated safety profile in pregnant women. There are currently no licensed vaccines that protect against GBS disease. Neurodevelopment Impairment after Infant GBS DiseaseGBS is a leading cause of infant meningitis, and almost one-fifth of GBS meningitis survivors experience moderate to severe neurodevelopment impairment (30). There is an additional, as yet unquantified burden associated with other invasive infant disease, such as GBS sepsis. It is critical to look toward improving the health and well-being of survivors of infant GBS disease, and supporting their families, for whom there are financial, social, psychological, and emotional impacts. See figure 4 below. 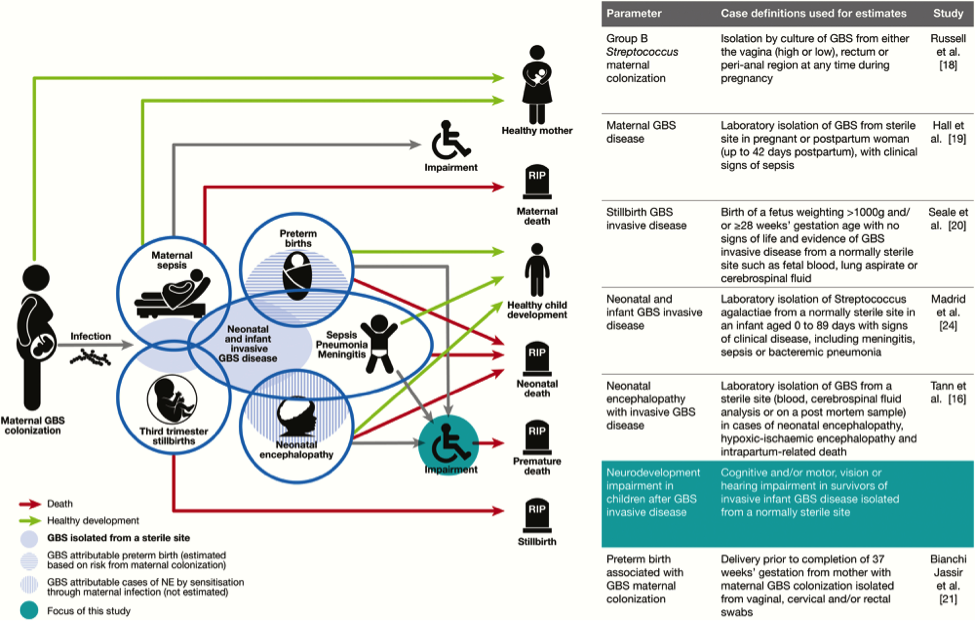 Meningitis and sepsis can cause brain injury in term and preterm infants. Magnetic resonance imaging (MRI) findings consistently show cerebrovascular involvement, and abnormal findings on neonatal MRI have been clearly associated with poor neurodevelopment outcome at 2 years (30). This study found that all 9 cases of infant GBS meningitis in term babies had abnormal Rate of suspected neonatal sepsis after cervical ripening with a transcervical Foley catheter: Mechanical cervical ripening by transcervical Foley catheter is a common method of labor induction in cases of unfavorable cervix, and its efficacy and safety have been confirmed in multiple studies during the past decades (31). Nevertheless, it is unknown whether colonization with GBS affects the risk for maternal and neonatal infection in women undergoing cervical ripening with transcervical Foley catheter. This study reports the rates of maternal and neonatal infection morbidity after cervical ripening for labor induction with transcervical Foley catheter in women with GBS colonization (32). The rate of suspected neonatal sepsis was 5.4% slightly higher than described before in other works not related to GBS colonization, possibly due to a different definition for neonatal infection. This work suggests a generally favorable outcome with the use of transcervical Foley catheter in women with GBS colonization, although larger comparative studies are required to further improve counseling for this unique risk group. GBS, a common commensal in the gut of humans and in the lower genital tract in women, remains an important cause of neonatal mortality and morbidity. The incidence of early onset disease has fallen markedly in countries that test women for carriage at 35 - 37 weeks of pregnancy and then offer intrapartum prophylaxis with penicillin during labor. Countries that do not test, but instead employ a risk factor approach, have not seen a similar fall. There are concerns about the effect on the neonatal microbiome of widespread use of antibiotic prophylaxis during labor, but so far the effects seem minor and temporary. Vaccination against GBS would be acceptable to most women and GBS vaccines are in the early stages of development. While most babies recover from their GBS infection, some are stillborn, more die in the first weeks of life and others suffer lifelong disability. Despite efforts of many developed countries to prevent these infections, which are not preventable using current risk-based or screening strategies. Prevention strategies (intrapartum antibiotic prophylaxis) for early-onset invasive infant GBS disease are currently limited to developed countries, and only around the time of birth. Maternal GBS vaccination may be able to reduce the burden of GBS disease further, particularly GBS meningitis, which mainly presents as late-onset disease beyond 7 days of life. |