


Breast Cancer Surgical Treatment Complications & Lymphedema
WHEC Practice Bulletin and Clinical Management Guidelines for healthcare providers. Educational grant provided by Women's Health and Education Center (WHEC).
Complications after any operation can be minimized with thorough preoperative evaluation, meticulous technique, hemostasis, and wound closure. In addition to the standard oncologic evaluation, preoperative evaluation includes assessment of the patient's overall physiologic condition, with particular emphasis on tolerability of anesthesia, uncontrolled diabetes, hypertension, anemia, coagulopathy, or steroid dependency. Lymphedema is a dreaded complication of breast cancer surgery. Patients with severe lymphedema have chronic, often debilitating arm swelling with resultant pain, decreased function, decreased quality of life, and cosmetic deformity. Because of its chronic nature, as well as a lack of proven long-term treatment methods, development of lymphedema is perhaps the most feared complication of breast cancer surgery for both patients and surgeons. Effective treatment for lymphedema is available. Early diagnosis is important since treatment is most effective when lymphedema is diagnosed at the earliest stage. Every patient with lymphedema should have access to established effective treatment for this condition. Lymphedema has no cure but can be successfully managed when properly diagnosed and treated.
The purpose of this document is to review commonly used approaches for the care of the post-mastectomy wound and addresses the complications encountered in these patients. Rehabilitation of the post-mastectomy patients produces problems of varying complexity. Pathophysiology, prevention, and management of lymphedema are also discussed. Mastectomy is a safe operation with low morbidity and mortality. Although the incidence of postoperative complications is low, physicians should be aware of the morbidity unique to mastectomy and axillary node dissection. The risk of developing lymphedema does not diminish over time but is a lifelong risk. Progressive lymphedema is complicated by recurrent infections, non-healing wounds, discomfort or pain, difficulty with daily tasks, emotional and social distress.
Care of the Post-mastectomy Wound
Technique at operation and wound closure is an essential part of wound repair. Meticulous hemostasis must be confirmed before closure. Closed-suction drains should be placed into the mastectomy wound site, because most patients will develop a seroma. We prefer closed-suction catheter drainage of the mastectomy wound, commercially available as Blake (Ethicon) or Jackson-Pratt tubing (Baxter) and each system should be placed appropriately at operation to allow superomedial and inferolateral positioning to ensure thorough, dependent aspiration. After the wound is closed, the tubing is connected to ensure removal of all wound contents (e.g., clots, serum). Suction catheter drainage, as a rule, is necessary for 5 to 10 days postoperatively. Routinely, catheters are removed only when less than 30 ml of serous or serosanguineous drainage is evident for two consecutive 24-hour intervals.
The skin is closed in two layers using absorbable suture. A light, dry gauze dressing is applied to the incision. Pressure dressings over the dissected skin flaps are unnecessary and do not decrease the amount and rate of seroma formation (1). Postoperatively, the wound is carefully inspected with regard to flap adherence, and the patient is encouraged to resume preoperative activity. In most circumstances, the breast cancer patient is allowed to begin the gradual resumption of pre-surgical activities. Younger women usually regain full range of motion of the arm and the shoulder soon after drain removal, whereas some older patients may require intense (supervised) exercise for several months before attaining their former levels of activity. Home-visits from the healthcare providers of the Visiting Nurse Association (VNA) are of particular value for psychosocial and physical recovery of post-mastectomy patient. Breast reconstruction is an important adjunct in the treatment of breast cancer. The advantages of breast reconstruction in terms of quality of life are well documented (2). In addition, recent studies have disproven many of the concerns regarding the potential effects of breast reconstruction on breast surgery management (3). For instance, large series have shown that breast reconstruction does not alter the biologic behavior of breast cancer, does not significantly delay or interfere with administration of adjuvant chemotherapy, and is not associated with a delay in the diagnosis of breast cancer recurrence (4). However, despite the fact that breast reconstruction is now performed routinely, there is no data regarding the impact of breast reconstruction on the development of lymphedema.
Complications of Mastectomy
- Wound Infection: After modified radical mastectomy the rates of wound infections range from 2.8% to 15% (5). Infection of the mastectomy wound or ipsilateral arm may represent serious morbidity in the postoperative patient and produces disability that may progress to late postoperative lymphedema of the arm. Cellulitis seen in the early post-operative period, responds to antibiotic treatment in most cases. When abscess formation does occur, attempts should be made to culture the wound for aerobic and anaerobic organisms with immediate Gram-stain of identifiable strains to document the bacterial contaminant. The predominant organisms are S aureus and S epidermidis. Factors that may increase the risk for infection include open biopsy before mastectomy, increasing age, prolonged suction catheter drainage, and alterations of host defense mechanisms.
- Seroma: It is a collection of serous fluid within a surgical cavity that is clinically evident. After mastectomy, seromas occur in the dead space beneath the elevated skin flaps and represent the most frequent complication of mastectomy, developing in approximately 30% of cases (6). With surgical ablation of the breast, the intervening lymphatics and fatty tissues are resected en bloc; thus the vasculature and lymphatics of the gland are transected. Therefore, transudation of lymph and the accumulation of blood in the operative field are expected. Operative technique should minimize lymphatic spillage and transudation of serum to allow rapid adherence of the skin flaps to deep structures without compromise of blood flow to skin flaps or the axilla. The use of closed-system suction catheter drainage over the last 20 years has greatly facilitated the reduction in protracted serum collections. Patients with a higher body mass index (BMI) have an increased rate of seroma formation. The incidence of seroma formation also increases with age (7). Most oncology surgeons recommend -- allowing arm mobility immediately after surgery but delay a structured exercise routinely until after the drains have been removed.
- Pneumothorax: It is rare complication, develops when the surgeon perforates the parietal pleura with extended tissue dissection or with attempts at hemostasis for perforators of the intercostals musculature. Pneumothorax is more commonly seen in patients undergoing a radical mastectomy after removal of the pectoralis major musculature. Respiratory distress is recognized in the operative or the immediate post-operative periods and pneumothorax is confirmed with a chest X-ray. Immediate intervention with closed thoracostomy drainage of the pleural space is essential as soon as pneumothorax is verified.
- Tissue Necrosis: A commonly recognized complication of breast surgery is necrosis of the developed skin flaps or skin margins. Bland and colleagues observed an incidence of 21% for minor and major necrosis of mastectomy skin flaps with associated wound infection (7). Local debridement is usually not necessary in minor areas of necrosis (<2 cm area). Larger areas of partial or full-thickness skin loss require debridement and on occasion the application of split-thickness skin grafts. Rotational composite skin flaps and subcutaneous skin tissue can be used from the lateral chest wall or the contralateral breast to cover the defect.
- Hemorrhage: It is reported as a post-operative complication in 1% to 4% of patients and is manifested by undue swelling of flaps of the operative site (8). Early recognition of this complication is imperative. Aspirating the liquefied hematoma and establishing patency of the suction catheters can treat hemorrhage. The application of a light compression dressing reinforced with Elastoplast-tape should diminish the recurrence of this adverse event. Early severe hemorrhage is most often related to arterial perforators of the thoracoacromial vessels or internal mammary arteries. Direct suture ligation is advisable. Miller and associates concluded that use of the electrocautery for the development of skin flaps in the performance of a mastectomy reduces blood loss without incurring a greater incidence of wound complications (8).
- Neuro-Vascular Structures Injuries: Injury to the brachial plexus is a rare complication of mastectomy and avoided by meticulous (cold scalpel) sharp dissection in and about the neuro-vascular bundle and through the development of tissue planes that parallel the neurilemma and the wall of the axillary vein to allow en bloc resection of lymphatic structures and fatty tissue. The sensory innervation of the breast is derived from the lateral and anterior cutaneous branches of the second through the sixth intercostals nerves. The patient usually experiences moderate pain in the operative site, shoulder, and arm in the immediate postoperative period. Because of the necessity of extensive flap development, the patient may note hyperesthesia and paraesthesia, as well as occasional "phantom" hyperesthesia in the mastectomy site. Phantom breast syndrome is a continued sensory presence of the breast after it has been removed. It is a phantom pain in 17.4% of cases, and in 11.8% of cases, and it presents as a non-painful phantom sensation such as itching, nipple sensation, and premenstrual-type breast discomfort (9).
Less common are injuries to the thoracodorsal nerve and the long thoracic nerve (respiratory) of Bell. The thoracodorsal, or subscapular, nerve innervates the lattissimus dorsi muscle in its course with the thoracodorsal (subscapular) vessels and is commonly sacrificed when lymphatics are discovered to be involved with metastases at axillary dissection. Injury or transaction of the long thoracic nerve of Bell produces instability and unsightly prominence of the scapula ("winged scapula"). The patient sustaining such an injury will often complain of shoulder pain at rest and with motion for many months after the procedure. All attempts should be made to preserve this nerve, yet its involvement with invasive neoplasm or nodal extension may require that it be sacrificed to ensure adequate en bloc extension. The lateral and medial pectoral nerves to the pectoralis major muscles and the motor innervation to the pectoralis minor exit the brachial plexus to enter the posterior aspects of these muscles in proximal axilla. Preservation of the pectoralis major and its function is the objective of the modified radical mastectomy. Thus maintenance of the integrity of the medial and lateral pectoral nerves is paramount to ensure subsequent function of the pectoralis major.
Lymphedema
Lymphedema is caused by an abnormality of the lymphatic system leading to excessive build up of tissue fluid that forms lymph, known as interstitial fluid. Stagnant lymph fluid contains protein and cell debris that causes swelling of affected tissues. Lymph is responsible for transporting essential immune chemicals and cells. Lymphedema is the accumulation of protein-rich fluid in soft tissues as a result of interruption of lymphatic flow. It occurs most frequently in the extremities, but it can also be found in the head, neck, abdomen, lungs, and genital regions. In post-mastectomy patients, chronic lymphedema has the potential to become a permanent, progressive condition. If it is allowed to progress, the condition can become extremely treatment resistant and in most cases cannot be completely relieved with either medical or surgical means. Left untreated, lymphedema leads to chronic inflammation, infection and hardening of the skin that, in turn, results in further lymph vessels damage and distortion of the shape of affected body parts (11). Interstitial fluid can build up in any area of the body that has inadequate lymph drainage and cause lymphedema. Lymphedema is a condition that develops slowly and once present is usually progressive (12). Lymphedema is divided into two forms: primary lymphedema and secondary lymphedema. People can be born with abnormalities in the lymphatic system. This type of lymphedema is known as primary lymphedema. Depending on how severe the condition is, swelling can be present at birth or may develop later in life. Primary lymphedema is associated with developmental abnormalities of the lymphatic system, may be manifested in neonates (congenital), adolescents (praecox), or patients older than 35 years (tarda). Secondary lymphedema is the most common form of lymphedema. This usually occurs after oncologic surgery or radiation therapy. The condition occurs as a result of damage by metastatic disease to the lymphatic system, post-radiation changes to the underlying skin structures, or surgical removal of one or more lymphatic nodal basins. Most lymphedema in the United States is secondary lymphedema. This type of lymphedema occurs from damage to the lymphatic system, commonly from cancer and its treatment but also from trauma to the skin such as from burns or infections (13). Lymphedema after breast cancer has been studied the most, but lymphedema can occur as a result of other cancers, including melanoma, gynecologic cancer, head and neck cancer or sarcoma.
It is estimated that as many as 30%-50% of all patients who undergo axillary lymph node dissection go on to develop some form of lymphedema (10). Variability in the reported incidence of lymphedema is due in part to the lack of a standardized definition (14). In addition, although most patients who develop lymphedema do so within 3 years of surgery, the onset of lymphedema occurs up to 25% of patients (10). In addition to measured arm swelling, many patients have perceived or subjective arm swelling that is difficult to quantify (15). Advances in the management of breast cancer, most notably the advent of sentinel lymph node biopsy (SLNB), have decreased the incidence of lymphedema. However, recent long-term studies have shown that even in patients undergoing SLNB alone, both objectively and subjectively measured lymphedema can occur in 3%-5% (15)(16). Thus, it is clear that even the minor perturbations in axillary drainage patterns that occur with SLNB can in some cases cause lymphedema.
Contributing Factors of Lymphedema
Six contributing factors have been shown to influence the incidence of brachial edema after treatment for breast cancer: radiation therapy; obesity; age; operative site; incision type and history of infection. Adding radiation therapy has been shown to increase the incidence of lymphedema from 20% to 52% (17). The incidence of lymphedema is lessened if transverse rather than oblique incisions are used (18). The extent of axillary dissection is an important contributing factor. Limiting the axillary dissection to level I and II nodes and preserving the level III nodes and lymphatic collateral channels around the shoulder may decrease the incidence of acute and chronic lymphedema. Recent technology has introduced the concept of lymphatic mapping and SLNB for women with invasive breast cancer. With the hypothesis that the histology of the SLNB reflects the histology of the remaining nodes in the basin, full nodal staging information can be garnered with a simple lymph node biopsy of one or more nodes. This approach may limit the possibility of lymphedema to only those women with histologic evidence of metastatic disease in the axilla.
Chronic lymphedema is a significant problem with limited treatment options (19). In the United States, the most common cause of lymphedema is axillary lymph node dissection for breast cancer (19). Most authors categorize arm swelling greater than 5 cm from baseline/contralateral arm or as volume difference of greater than 40% from baseline as severe lymphedema (17)(20). Moderate lymphedema is usually defined as 2-5 cm arm circumference increases. Some authors have defined mild lymphedema as differences in arm measurements that are less than 2 cm but are associated with subjective sensation of swelling. The use of patient perception in the definition of lymphedema is important and is advocated by the American Cancer Society (ACS). As such, patient-directed interviews and validated instruments that assess lymphedema symptoms have been developed and enable combination of patient perception and objective measurements (21). The onset of lymphedema relative to surgical intervention is unpredictable and may occur over several years. Large clinical series have identified a number of risk factors for lymphedema. The most consistently identified risk factors include obesity, postoperative weight gain, postoperative surgical site/arm infections, and radiation therapy to the axilla (22).
Staging of Lymphedema
Stage I:
- Characterized by pitting edema and is reversible with elevation of the arm.
Stage II:
- Edema is no longer spontaneously reversible;
- Development of protein-rich edema;
- Proliferation of fibrotic tissue.
Stage III:
- Known as elephantitis;
- Massive swelling of the extremity;
- Protein-rich fluid;
- Connective and scar tissue;
- Hardening of the dermal tissue;
- Papillomatosis.
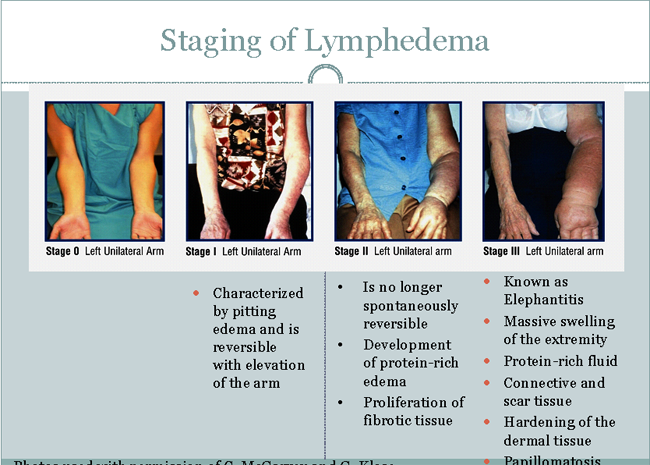
Fig. 1. Staging of Lymphedema
Diagnosis and Symptoms
Diagnosis can be established on the basis of an accurate history and a thorough physical examination. Assessment of the progression of edema is essential in the postoperative care of patients. Photography at preoperative and postoperative visits can be very useful in determining the onset and progression of lymphedema. Circumferential measurements using reference points to bony landmarks may also be a practical and simple way to follow patient's lymphedema. Differences in circumferential measurement between two opposing limbs are noted at multiple landmarks. These measurements are totaled for each limb and compared. If there is a difference of greater than 10 cm, lymphedema exists. Water displacement is the most accurate method of documenting changes in edema. This would appear to be the best objective criterion with which to judge lymphedema and response to therapy. However, these techniques are time consuming and are limited to facilities that have the equipment to perform study. Bioelectrical impedance techniques are the most recent developments for evaluating accumulation of fluid in affected extremities. Symptoms of chronic lymphedema are usually elicited by taking an accurate history of the patient. Patients complain of an overall increase or "fullness" of the extremity, with a corresponding "heaviness" and decreased functional ability.
Soft Tissue Imaging: Magnetic resonance imaging (MRI), computed tomography (CT) and some types of ultrasound (US) are able to detect the presence of extra fluid in the tissues (23). Fluid that is outside the cells (extracellular) and also outside the vessels (extravascular) is called tissue fluid or interstitial fluid. Lymphedema is one type of interstitial fluid build-up that occurs when fluid is not being removed by the lymph vessels. MRI, CT and US can show the presence of increased interstitial fluid but cannot tell the cause. These imaging techniques have to be put together with history, physical examination and sometimes other imaging tests. Other conditions such as heart failure or low proteins in the blood from liver disease or malnutrition can cause fluid to build up in the tissues. MRI, CT scans and US may be required to determine the cause of lymphedema, especially if there is a concern that the lymphedema might be the result of an untreated cancer.
Lymph Vessel Imaging: Lymphoscintigraphy is a nuclear medicine study used for imaging lymph vessels and lymph nodes (24). Radio-labeled particles of protein are injected just under the skin of the area of the body to be imaged. Usually technetium labeled sulphur colloid is used. Lymphoscintigraphy is accurate for detecting abnormalities of the lymphatic system in the extremities regardless of the cause. It demonstrates slow or absent lymph flow and areas of reflux (backflow). It can reveal abnormalities of lymph intake in lymph nodes with some forms of lymphedema. It predicts response to treatment and shows the main, larger lymph vessels, basic architecture of the peripheral lymphatic system and nodes (24). It does not show the deep transport lymph vessels carrying lymph from the nodes back to the blood circulation. Lymphoscintigraphy identifies lymphatic abnormalities at a late stage, after lymphedema has occurred. A new technique for imaging lymph vessels is Near Infra-Red Florescence Imaging (NIR) using a substance known as indocyanine green (ICG) (25). The ICG is injected into the skin and immediately imaged with a dynamic (real time) infrared florescence camera. With NIR-ICG, even very small lymphatic vessels can be seen. It can diagnose lymphedema and find abnormalities at an early stage, possibly before swelling is obvious. Although this technique shows promise for the diagnosis of lymphedema, it is currently available at very few centers, most of which are involved in research.
Measures of Volumes: Measures of limb (arm and leg) volume have been the standard way of detecting lymphedema for years and have been shown to be accurate when properly done (26). Volume is measured by 3 main methods: tape measurement, perometry, and water displacement. Tape measurements are taken at defined intervals, using geometric formulas to calculate the total volume. This technique can be accurate if it is done in precisely the same way each time, and is most accurate when the same person takes the measurements each time. Perometry uses an infra-red optical electronic scanner and computer to calculate the volume of the body part. Perometry is accurate if the body part is positioned exactly the same way each time and the machine has been calibrated for accuracy. Perometry has been demonstrated to detect as little as a 3% change in limb volume in breast cancer survivors followed over time (27). Water displacement, the bench "gold standard" for assessing volume, is rarely used these days due to its inconvenience.
Electrical Conductance Testing: Bioimpedance Spectroscopy (BIS) is a method for measuring water content in tissues. It has been used for many years to assess the total water content of the body and body composition for fitness and weight loss purposes. BIS is now available to measure interstitial fluid as a component of assessment leading to the diagnosis of lymphedema and has been shown to provide reliable data to be used in the diagnosis of breast cancer-related lymphedema (28). BIS is done by passing a small, painless, electrical current through the limb and measuring the resistance to current (impedance). The machine uses certain electrical current frequencies to determine if more fluid exists as compared to the contralateral limb. It does this comparing the difference in resistance to electricity passed through interstitial fluid compared to intracellular fluid. BIS currently is done on the whole limb since the resistance to current flow for standard technique is calculated to the length of the body part. The higher the water content in the interstitial tissue, the lower the resistance (impedance). BIS is not accurate in advance, fibrotic edema.
Changes in Biomechanical Properties of Tissues: These measures of the biomechanical properties of tissues are important for research. Hopefully continued development will lead to better tools for clinical use so that diagnostic methods will include quantitative methods of skin and subcutaneous tissue changes associated with progressive lymphedema. Lymphedema causes the affected skin and subcutaneous tissues to become inflamed and hardened (fibrotic). Currently, these skin changes are documented by physical examination of tissue texture, pitting, enlarged skin folds and other dermatologic conditions such as wounds and papillomas (benign growths on the skin in areas of lymphedema). Methods available for measuring skin texture and resistance quantitatively are: tissue dielectric constant and tonometry (29).
Importance of Early-Lymphedema Screening
Typically, lymphedema is diagnosed only when it is visually apparent, at which point treatment is often ineffective. The focus of WHEC Cancer Center's screening program is to diagnose the condition in its subclinical state when early intervention can prevent development of clinical signs and symptoms. The baseline measurement and periodic measurements after treatment of breast cancer are vital to accurate diagnosis. The measurement takes just three minutes using a perometer -- device that employs infrared technology to accurately verify arm volume. Arm measurement, which is now a part of standard clinical evaluation has helped us better identify and treat the condition and also has led to greater understanding of the risk factors involved. Early interventions such as wearing a compression sleeve for 12 weeks can prevent progression of the condition. Women who progress to moderate lymphedema are managed by more aggressive measures such nightly bandaging, massage and compression, in addition to wearing a sleeve, are beneficial. Some women experience a transient form of the condition; they show signs of subclinical lymphedema but do not progress to clinical symptoms. Distinguishing the two groups is critical to ensuring that women do not receive unnecessary treatment (40). In this study, the researchers have determined that undergoing lymph node dissection or radiation to the lymph nodes increases a woman's risk of developing lymphedema. Up to 8% of patients who have sentinel node biopsies and 20 to 25% of women with axillary lymph node dissection develop lymphedema at some time after treatment (40). Adjuvant radiation therapy and postoperative infection increase the risk of developing lymphedema, as does having a body mass index of more than 25.
n
Fig. 2. A potentially irreversible form of disfiguration, lymphedema can hinder arm function and is often diagnosed too late for treatment to be effective. The women pictured above experienced arm volume increases of 31% (A) and 54% (B).
Treatment Options
- Prevention: The radical mastectomy of the past has been replaced with more conservative procedures that have the potential for decreasing the incidence of lymphedema. The new technique of lymphatic mapping and sentinel lymph node biopsy promises to provide full nodal staging information with a simple lymph node biopsy. Lymphedema should be non-existent after this procedure. Primary healing creates less fibrosis than does scarring by secondary intention. Attention to detail and good surgical techniques of sharp dissection, adequate hemostasis, suction drainage, and closure without tension should lessen the chance of postoperative lymphedema. Wound infection and sepsis should be avoided, suggesting a role for perioperative antibiotics. Radiation therapy after lumpectomy should not include axilla, unless the chance of recurrence in the axilla is overwhelming. If axillas are included in the radiation field, the incidence of lymphedema may be as high as 52% (30).
- Medical Treatment: The initial treatment of chronic secondary lymphedema should be managed through non-surgical measures. Physical therapy, in conjunction with compression garments or sequential-gradient compression-type pumps, has been recently added to the overall care of patients with chronic lymphedema. Medical management should involve a multidisciplinary approach in the patient's long-term care. This includes patient education, instruction in home physical therapy exercises, maintenance of normal range of motion and strength in the affected extremity, and preservation of existing motion.
Lymphedema Checklist Guidelines (30):
DO:
- Do Keep skin clean
- Do moisturize skin
- Do elevate limb while sleeping and traveling
- Do wash with hypo-allergenic soaps and cleaners
- Do use electric not straight razors to remove hairs
- Do use mild detergents for clothes
- Do keep temperature in house constant
- Do eat a balanced nutritional diet
- Do treat infections early and throughout with antibiotics prescribed by your doctor
- Do exercise: walk, swim, prescribed isometrics
- Do wear prescribed garments and/ or bandages
- Do avoid cuts, burns, and insect bites
- Do avoid sunburn -- use sun-block
- Do wear loose-fitting clothing
DO NOT:
- NO PROCEDURES SHOULD BE PERFORMED ON THE AFFECTED EXTREMITY.
- No blood drawing
- No injections
- No intravenous dye x-ray studies
- No acupuncture
- No liposuction
- No blood pressure testing
- No heavy, traumatic, or repetitive exercises
- No picking up heavy objects
Complete Decongestive Therapy (CDT)
It is also called Combined, Complex or Comprehensive Decongestive Therapy (CTD). It is the main treatment of lymphedema and is considered "gold standard" of treatment. CDT has been shown to be effective and safe. It consists of an initial reductive phase (Phase I) followed by a maintenance phase (Phase II) (31). In Phase I, the main goals are reducing the size of the affected part and improving the skin. After Phase I, the person with lymphedema needs to continue into Phase II, an ongoing, individualized self-management phase to make sure the gains of Phase I are maintained long-term. Components of CDT are: manual lymph drainage; multi-layer, short-stretch compression bandaging; lymphatic exercise; skin care; education in lymphedema self-management, and elastic compression garments. Effects of CDT are to: decrease swelling; increase lymph drainage from the congested areas; reduce skin fibrosis and improve the skin condition; enhance patient's functional status; relieve discomfort and improve quality of life; reduce the risk of cellulitis and Stewart-Treves-Syndrome, a rare form of angiosarcoma.
Optimally, Phase I CDT is performed daily (5 days/week) until the reduction of fluid volume has reached a plateau, which can take 3 to 8 weeks (31). Some patients may have good results from CDT with modifications of the frequency and duration of treatment. CDT frequency and duration should be individualized to produce the greatest reduction of swelling and improvement of skin condition in the shortest period of time. At the completion of Phase I CDT, the person with lymphedema is set up on a self-management program that includes self-lymph drainage (sometimes called Simple Lymphatic Drainage), home lymphatic exercises, a skin care regimen, and compression garments or bandages that the individual learns to apply. Some individuals may require additional measures with Velcro, specialized foam construction garments, and pneumatic compression devices. Phase II maintenance must be monitored and changed periodically, just as treatment for any other chronic medical condition. Compression garments must be replaced every 4-6 months to be effective. Specialized equipment requires maintenance and replacement according to manufacturers' guidelines. Phase II CDT and periodic medical monitoring are essential to the long-term success of lymphedema treatment. Diuretics are of minimal aid in the treatment of chronic lymphedema resulting from oncologic surgery or metastatic spread of the disease. Compression pumps are rapidly becoming a major factor in medical management of patients with chronic lymphedema. Researchers have recently focused attention on recreating the beneficial effects of massage through mechanical or compressional means, leading to the development of compression devices. These compression machines are based on two basic principles. The first is the single-cell compartment system providing absolute pressure. These devices offer no direction for fluid transport, which causes some backflow of lymphatic fluid. The second-generation devices are multi-cell systems based on sequential compression of the extremity. It delivers compression at the same pressure in each garment section from distal to proximal. However, this does not imitate the normal muscular and vascular activities of an extremity. Few drugs are being studied for treatment of chronic lymphedema. Benzopyrones can decrease the overall volume of high-protein-concentrate edema by stimulating proteolysis. Venalot, a benzopyrene is a drug that breaks down large protein molecules, facilitating absorption of the proteins into the vascular system at the level of the capillaries (32).
Intermittent Pneumatic Compression Therapy (IPC)
IPC, also known as compression pump therapy, can be useful in some patients as an adjunct to Phase I CDT or a necessary component of a successful home program for Phase II CDT (33). Acceptable pumps should have appliances (pump garments) with multiple chambers and have a sequential pressure delivery with the chambers compressing in a specific pattern determined individually for the patient's diagnosis and pattern of lymphedema. Recommended pump pressures generally range from 30-60 mmHg, although lower or higher pressures may be indicated. In general, lower pressures are considered to be safer, but the pressure has to be individualized to the patient's diagnosis and skin condition. The length of each treatment is usually one hour. IPC is not a "stand alone" treatment. It is utilized along with standard CDT to maintain control of lymphedema at home. To maintain edema control, a compression garment, or short-stretch bandages, should be worn between pump treatments and also when IPC therapy is discontinued. Patients being considered for IPC must be evaluated by a physician or healthcare provider with expertise in lymphedema. It is important to insure safe selection of the proper device and appropriateness of IPC. The prescription must include the intensity of pressure and pattern of pressure needed, taking into consideration several aspects of patient's situation including determination of need for programmable pressure to treat fibrotic areas, address treatment of ulcers, and adjust for patient's level of pain and skin sensitivity (34). If trunk, chest or genital swelling is present, the physician must determine whether a pump that provides appliances to treat those areas is necessary or if the patient can manage the trunk swelling through self-manual lymph drainage or garments. If a pump with only extremity attachments is used, close monitoring should be instituted to detect an increase in edema or fibrotic (hard) tissue above the device sleeve, called a fibroscelerotic ring. If this occurs, consideration should be given to using a device that treats the trunk in addition to the extremities. Additionally, the physician or healthcare provider must evaluate the impact of various other medical conditions that are usually considered contraindications for pneumatic compression therapy, including acute infection, severe arterial vascular disease, acute superficial or deep vein phlebitis (inflammation or clot), recurrent cancer in the affected area, or uncompensated congestive heart failure.
Surgical Treatment
Surgery for lymphedema is not curative, but it has been used in specific circumstances for control of a severe condition. Circumstances where surgery may be considered are: reducing the weight of the affected limb, minimizing the frequency of inflammatory attacks, improving cosmetic appearance, or fitting the limb into garments. Surgical treatment should be instituted for patients for whom previous medical modalities have failed or for those who have had long-term complications. There are several types of surgical procedures available that have been used for lymphedema: (a) excisional operations, including debulking and liposuction, (b) tissue transfers, and (c) microsurgical lymphatic reconstruction. Previous studies have demonstrated that wound infections and infections of the ipsilateral arm are significant risk facts for the development of lymphedema. Many clinicians presume immediate breast reconstruction to increase the risk of lymphedema as a consequence of increased potential for surgical site infection. In this series (35), immediate reconstruction was not associated with increased risk of infection. Additionally, those patients who did have infections did not have an increased risk of lymphedema. This last observation must be interpreted with caution. However, as only a small number of patients in the current series had infections complications, thereby limiting the statistical power. In conclusion the study has shown that breast reconstruction with tissue expander following mastectomy does not increase the risk of lymphedema. This information is important for patient counseling.
Debulking: It removes the hard connective tissue and any large folds of fatty tissue associated with the lymphedema-affected body part (36). The potential risks of this surgery include prolonged hospitalization, poor wound healing, nerve damage or loss, significant scarring, destruction of the remaining lymphatic vessels in that body part, loss of limb function, return of swelling, poor cosmetic results, and decrease in quality of life. Postoperatively, compression garments are still necessary for the maintenance of the limb and must be worn life-long due to the lymphatic scarring from these surgeries and lymphatic insufficiency. Liposuction for lymphedema is similar, but not exactly the same, as cosmetic liposuction. The risk of liposuction include bleeding, infection, skin loss, abnormal sensation (such as numbness, tingling, "pins and needles" feeling), and lymphedema returning.
Microsurgical Lymphatic Reconstruction: There are new micro-surgical techniques that are currently being attempted using either lymphatic-venous shunts (LVSs) or lymphatic-venous anastomosis (LVA). These procedures allow a lymphatic egress of fluid into the venous circulation. They are done in conjunction with multiple limb fasciotomies and can improve lymphatic drainage through muscles and deep lymphatic circulation. Complications include thrombophlebitis and lymphangitis (37). Patients with diffuse interstitial fibrosis, the more traditional option of total superficial lymphangiectomy (Servelle's) or partial superficial lymphangiectomy (Kondoleon's) is recommended. An alternative microsurgical technique described by Campisi, Boccardo, and Tacchella involves performing interposition autologous lymphatic-venous-lymphatic (LVL) anastomosis. This procedure represents an alternative to direct LVSs and is based on the abundance of large-caliber venous tributaries. The LVL anastomosis consists of inserting suitably large and lengthy autologous venous grafts between lymphatic collectors above and below the site of obstruction to lymphatic flow. Contraindications to this procedure include lymph node hyperplasia or aplasia and extensive obliteration of superficial and deep lymphatic collectors. Reductions in limb volume have been reported and a number of preliminary studies have been done, but there are no long-term studies of the effectiveness of these techniques (38).
Complementary, Integrative and Alternative Treatments
A number of promising treatments have been reported, but they have not yet been subjected to sufficient rigorous research to recommend as the standard of care. These treatments include cold laser, electrical stimulation, vibratory therapy, oscillation therapy, endermologie and aqua-lymphatic therapy (39). All of these techniques are done in combination with components of CDT. Acupuncture has shown benefit for some symptoms of cancer and cancer treatment, including fatigue, hot flashes, muscular or joint pain, neuropathy and nausea. There are no rigorous studies on using acupuncture for treating lymphedema or using acupuncture on lymphedema extremities (39). Rebounder trampolines have been advocated by some for treating lymphedema, but there are no published studies on this treatment. Rebounding is good exercise, it but is not known to be superior to other forms of aerobic exercise in individuals with lymphedema. Due to potential interactions of natural supplements with prescription drugs and other negative side effects, patients should check with their physician or healthcare provider before taking any natural supplements.
Summary
An accurate knowledge of physiology and pathophysiology of lymphedema is necessary to understand the rationale of treatment techniques available. An accurate assessment of the degree of impairment should be established before initiating either short- or long-term care. Although surgical intervention and treatment have been tried in the past, the standard of care now is a conservative medical management. A multidisciplinary approach is needed to maximize available treatment regimens. Surgeons, nurses, physical and occupational therapists play active roles in the care of chronic lymphedema patients. Appropriate patient education and instruction in self-care are paramount in the long-term care of patients. A realistic approach to the long-term care of this condition coupled with therapeutic and emotional support can ensure a productive and less debilitating lifestyle to patients with chronic extremity lymphedema. There are currently no standardized criteria to define lymphedema. The vast majority of clinical series studying lymphedema have used arm measurements at various distances proximal and distal to the olecranon process. Tissue expander breast reconstruction in patients undergoing SLNB or SLNB and axillary lymph node dissection does not increase the risk of developing measured or perceived lymphedema. Treatment of lymphedema should be undertaken only after a thorough diagnostic evaluation has been done according to accepted guidelines by qualified practitioners. CDT has been shown to be effective in large numbers of case studies demonstrating limb volume reduction of 50-70% or more, improved appearance of the limb, reduced symptoms, improved quality of life, and fewer infections after treatment. Even people with progressive lymphedema for 30 years or more; starting CDT have been shown to respond. All interventions for lymphedema must have the goals of inducing and maintaining volume reduction, preventing medical complications, improving skin condition, reducing infection, enhancing patient adherence, and improving comfort and quality of life.
Acknowledgement: Special thanks to Dr. Steven M. Schonholz, Medical Director, Breast Cancer Center at Mercy Medical Center, Springfield, MA (USA) for expert opinions and assistance in preparation of the manuscript.
References
- O'Hea BJ, Ho MN, Petrek JA. External compression dressing versus standard dressing after axillary lymphadenectomy. Am J Surg 1999;177:450-455
- Elder EE, Brandber Y, Bjorklund T, et al. Quality of life and patient satisfaction in breast cancer patients after immediate breast cancer reconstruction: a prospective study. Breast 2005;14:201-208
- McCarty CM, Pusic AL, Sclafani L, et al. Breast cancer recurrence following prosthetic, postmastectomy reconstruction: incidence, detection, and treatment. Plast Reconstr Surg 2008;121:381-388
- Howard MA, Polo K, Pusic AL, et al. Breast cancer local recurrence after mastectomy and TRAM flap reconstruction: incidence and treatment options. Plast Reconstr Surg2006;117:1381-1386
- Morrow M, Jagsi R, Alderman AK, et al. Surgeon recommendations and receipt of mastectomy for treatment of breast cancer. JAMA 2009;302:1551-1556
- Vinton AL, Traverso LW, Jolly PC. Wound complications after modified radical mastectomy compared with tylectomy with axillary lymph node dissection. Am J Surg 1991;161:584-589
- Banerjee D, et al. Obesity predisposes to increased drainage following axillary node clearance: a prospective audit. Ann R Coll Surg Engl 2001;83:268-272
- Miller PJ, et al. Scalpel versus electrocautery in modified radical mastectomy. Am Surg 1988;54:284-293
- Kroner K, et al. Long-term phantom breast syndrome after mastectomy. Clin J Pain 1992;8:346-354
- Petrek JA, Senie RT, Peters M, et al. Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis. Cancer 2001;92:1368-1377
- Foldi E, et al. The science of lymphedema bandaging in Caine, S. Editor. European Wound Management Association (EWMA). Focus Document: Lymphedema Bandaging in Practice. London: MEP Ltd, 2-4, 2005
- Lawenda B, et al. Lymphedema: A primer on the identification and management of chronic condition in oncologic treatment. Cancer Journal for Clinicians 2009:59:8-24
- Pillar N. Phlebolymphoedema/chronic venous lymphatic insufficiency: an introduction to strategies for detection, differentiation and treatment. Phlebology 2009;24:51-55
- Armer JM, Stewart BR. A comparison of four diagnostic criteria for lymphedema in a post-breast cancer population. Lymphat Res Biol 2005:3:208-217
- Mclaughlin SA, Wright MJ, Morris KT, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: patient perceptions and precautionary behaviors. J Clin Oncol 2008;26:5220-5226
- Mclaughlin SA, Wright MJ, Morris KT, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurement. J Clin Oncol 2008;26:5213-5219
- Segerstrom K, et al. Factors that influence the incidence of brachial edema after treatment of breast cancer. Scand J Plast Reconstr Surg Hand Surg 1992;26:223-229
- Cody HS III. The learning curve for sentinel lymph node biopsy in breast cancer. Arch Surg 2000;135:605-606
- Soran A, D'Angelo G, Begovic M, et al. Breast cancer-related lymphedema -- what are the significant predictors and how they affect the severity of lymphedema? Breast J 2006;12:536-543
- Sener SF, Winchester DJ, Martz CH, et al. Lymphedema after sentinel lymphadenectomy for breast carcinoma. Cancer 2001;92:748-752
- Armer J, Fu MR, Wainstock JM, et al. Lymphedema following breast cancer treatment, including sentinel lymph node biopsy. Lymphology 2004;37:73-91
- Hinrichs CS, Watroba NL, Rezaishiraz H, et al. Lymphedema secondary to postmastectomy radiation: incidence and risk factors. Ann Surg Oncol 2004;11:573-580
- Astrom K, et al. Imaging of primary, secondary and mixed forms of lymphedema. Acta Radiol 2001;42:409-416
- Szuba A, et al. Diagnosis and treatment of concomitant venous obstruction in patients with secondary lymphedema. J Vasc Intervent Radiol 2003;13:799-803
- Rasmussen J, et al. Lymphatic imaging in humans with Near-Infrared Fluorescence. Curr Opin Biotechnol 2009;20:74-82
- Hayes S, et al. Comparison of methods to diagnose lymphedema among breast cancer survivors: 6 month follow up. Br Ca Res Treat 2005;89:221-226
- Zuther JE. Lymphedema Management: The Comprehensive Guide for Practitioners. 2nd ed. New York, NY: Thieme; 2009
- Mayrovitz H. Suitability of single tissue dielectric constant measurements to assess local tissue water in normal and lymphedematous skin. Clin Physiol Imaging 2009;29:123-127
- Mayrovitz H. Assessing lymphedema by tissue indentation force and local tissue water. Lymphology 2009;42:88-98
- Bland & Copeland. The Breast: Comprehensive Management of Benign and Malignant Disorders. 3rd edition, Volume two. Pp 969; 2004. Publisher: Saunders; an imprint of Elsevier
- Mayrovitz HN. The standard of care for lymphedema: current concepts and physiological considerations. Lymphat Res Biol 2009;7:101-108
- Casley-Smith J, Morgan R, Piller N. Treatment of lymphedema of the arms and legs with 5,6-benzo- [alpha]-pyrone. N Engl J Med 1993;329:1158-1164
- Ridner S, et al. Home-base lymphedema treatment in patients with cancer-related lymphedema or non-cancer-related lymphedema. Oncol Nurs Forum 2008;35:671-680
- Olszewski W. Anatomical distribution of tissue fluid and lymph in soft tissues of lower limbs in obstructive lymphedema-hints for physiotherapy. Phlebolymphology 2009;16:283-289
- Avraham T, Daluvoy SV, Riedel ER, et al. Tissue expander breast reconstruction in not associated with an increased risk of lymphedema. Ann Surg Oncol 2010;17:2926-2932
- Salgado CJ, Sassu P, Gharb BB, et al. Radical reduction of upper extremity lymphedema with preservation of perforators. Ann Plast Surg 2009;63(2):302-306
- Campisi C, et al. Lymphatic microsurgery for the treatment of lymphedema. Microsurgery 2006;26(1):65-69
- Narushima M, et al. The intravascular stenting method for treatment of extremity lymphedema with multiconfiguration lymphaticovenous anastomosis. Plast Reconstr Surg 2010;125:935-943
- National Lymphedema Network. Position Statement of the National Lymphedema Network. http://www.lymphnet.org/lymphedemaFAQs/positionPapers.htm Accessed 15 July 2011
- Ancukiewicz M, et al. Standardized method for quantification of developing lymphedema in patients treated for breast cancer. Int J Radiat Oncol 2011;79(5):1436-1443
Published: 15 August 2011
Dedicated to Women's and Children's Well-being and Health Care Worldwide
www.womenshealthsection.com