


Psycho-Oncology Services for Gynecologic Cancer
WHEC Practice Bulletin and Clinical Management Guidelines for healthcare providers. Educational grant provided by Women's Health and Education Center (WHEC).
A cancer diagnosis is associated with a range of physical, psychological, social, and existential challenges. For some individuals, their personal or situational resources are not sufficient to manage these challenges, which in turn contribute to an array of adverse effects, including psychological distress. Much attention has been given to implementing routine screening programs in cancer care to improve the management of distress following diagnosis. Although patients might screen positive for distress, several studies have found that most then refuse additional psychosocial support. To inform the development of successful models of distress screening, the study at our institution and literature review revealed preferences for psychosocial care among women diagnosed a gynecologic cancer who scored at least 4 on the Distress Thermometer (DT). Many refused the referral to see a psychologist. Women typically reported that a referral was not needed, because their rating on the DT reflected transient stressors or physical distress. Many also spoke about their need to cope with the challenges they were facing on their own and the extensive social support they already had in place to help them overcome these challenges. Women who accepted referral to the psychologist often struggled to cope with several losses they felt had existential and long-term effects. Commonly, these women reported not having the social support they needed, managing several concurrent life stressors, and/or not having the repertoire of coping skills they required to "remain afloat".
The purpose of this document is to begin to bridge the gap between clinicians' and patients' expectations of how psychosocial services should be used in response to distress screening. The Women's Health and Education Center (WHEC) supports professional organizations with the mission to improve survival and quality of life for cancer patients through standard-setting, prevention, research, education and the monitoring of comprehensive quality care. This review begins to bridge the gap between healthcare providers' and patients' expectations of how psychosocial services should be used in response to distress screening. In 2014, the WHEC approved new standards to promote patient-centered care, an exciting shift driven by research over the past decade showing that patient-centered services improve outcomes. Patient-centered standards include the provision of treatment and survivorship plans, palliative care services, genetic services, navigation programs, and psychosocial distress screening.
Background
Psychological distress is a generic term that encompasses the spectrum of feelings from worry, vulnerability, and sadness, to depression, anxiety, and panic (1). Between 20% and 66% of patients with cancer report high levels of distress (2). Early identification and treatment of emotional-distress are important given its potential negative effects on patients' short- and long-term illness adjustment (3). Although distress is recognized internationally as the sixth vital sign, it often goes unrecognized because of health care professionals' lack of time and confidence in assessing distress. Throughout the past decade, much attention has been given to implementing routine distress screening programs in cancer care as a way of improving the management of distress. Routine distress screening at periods of increased vulnerability is now an integral part of international cancer control plans and best practice guidelines in psychosocial cancer care (4). Research increasingly supports the effectiveness of distress screening programs in identifying patients with adjustment disorders and of follow-up psychosocial care in improving psychological and physical functioning. However, despite the availability of psychosocial services, many patients who screen positive for distress do not accept referrals for further assessment or psychosocial services. These low rates of referral uptake often raise concerns among healthcare professional that patients are not receiving optimal cancer care.
Distress Thermometer (DT)
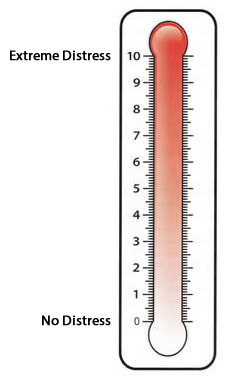
The DT is a single-item, 11 point visual analogue scale ranging from 0, denoting no distress, to 10, denoting extreme distress. DT is one of the best known tools for distress screening (5). In addition, several studies have supported its convergent validity with the hospital and anxiety depression scale. A cutoff score of 4 typically results in optimal sensitivity and specificity (6).
Opinions about DT
Reactions to being asked about distress: Unanimously, patients felt that completing the DT was appropriate, seeing it as part of the care they were receiving, regardless of whether they would then accept the referral for one-on-one counseling. The DT prompted them to consider their distress, and found it reassuring that someone was "out there looking after" their emotions. Patients expressed that it was easy to "ignore how you are actually feeling" when faced with the whirlwind of the diagnosis and treatment of gynecologic cancer. Similarly, all patients felt it was appropriate for psychologist to then follow-up and further assess their need for support (7).
Perceived usefulness of the DT: Across interviews, participants found the DT was useful in communicating their distress to their treating team, and connecting them to the services they might need. Some patients even if they do not accept the referral to see the psychologist, knowing that they are "in the system" usually is comforting and facilitates access to the service in the future, if needed.
Preferences for One-on-One Counseling: The main emphasis on accepting or refusing one-on-one counseling focuses on the type and length of stressors experienced, and their perceptions of their own internal and external resources to address these. Many times patients have been managing the life stressors, sometimes for many years (or decades), the cancer diagnosis may be the "breaking point". These patients are likely to accept the referral to see the psychologist, because they felt it was all becoming too much to bear, and they recognize that this additional pressure can put them at risk of exacerbation.
American College of Surgeons Commission on Cancer Psychosocial Distress Screening
- Psychosocial Distress Screening Standard 3.2 (8) - The cancer committee develops and implements a process to integrate and monitor on-site psychosocial distress screening and referral for the provision of psychosocial care.
- Timing - Patients with cancer are offered screening for distress a minimum of 1 time per patient at a pivotal medical visit to be determined by the program. Some examples of a "pivotal medical visit" include time of diagnosis, pre-surgical and post-surgical visits, first visit with a medical oncologist to discuss chemotherapy, routine visit with a radiation oncologist, or a post-chemotherapy follow-up visit. Preference is given to pivotal medical visits at times of greatest risk for distress, such as at time of diagnosis, transitions during treatment (e.g. from chemotherapy to radiation therapy), and transitions off treatment (9).
- Method - The mode of transmission (e.g. patient questionnaire, clinician-administered questionnaire) is to be determined by the program.
- Tool - Facilities select the tool to be administered to screen for current distress. Preference is given to standardized, validated instruments with established clinical cutoffs; however, facilities may use a measure of their choice. Facilities are encouraged to use established clinical cutoffs when possible; however, facilities may determine the cutoff score used to identify distressed patients (10).
- Assessment and referral - As recommended in the 2007 Institute of Medicine report, if clinical evidence exists of moderate or severe distress, the patient's oncology team (oncologist, nurse, social worker, and/or psychologist) is to "identify and examine the psychological, behavioral, and social problems of patients that interfere with their ability to participate fully in their health care and manage their illness and its consequences". This evaluation will confirm the presence of physical, psychological, social, spiritual, and financial support needs and indicate the need to link patients with psychosocial services offered on-site or through referral.
- Documentation - Screening, referral or provision of care, and follow-up are documented in the patient medical record to facilitate integrated, high-quality care.
Significance of Depression in Cancer
Depression extends beyond distress, which is a normal reaction of discomfort to stressors, many of which naturally accompany the diagnosis and treatment of cancer. Depression involves a negative turning inward, with feeling of hopelessness, helplessness, and worthlessness, with amplify the impact of stressors and impair response to them. The lethal potential of depression is underscored by a recent study indicating an elevated rate of suicide among patients with recently diagnosed cancer (11). The 1-year prevalence rates of depression among patients with cancer are between 15% and 29%, which are significantly higher than the 8.6% prevalence rate of major depression in the general US population (12).
Depression and cancer interact, with cancer increasing the likelihood of depression, and depression increasing the risk of cancer progression. Recent evidence shows that the inflammatory response to cancer and its treatment, including tumor cell lysis, elevates the levels of circulating cytokines that can include depressive symptoms, similar to the lethargy associated with acute infectious disease (13). The identification of depressive symptoms is crucial to directing treatment choice. Strong evidence shows that the psychotherapeutic treatment of depression, even among patients with advanced cancer, is highly effective (14). In addition, because comorbid depression predicts shorter survival time with cancer, there is good reason to think that treatment of depression may improve quantity and quality of life (15). Studies assessing depression over longer periods show that chronic depression is related to increased cancer risk and shorter subsequent survival (16). Depression may play a causal role in cancer mortality, and therefore its treatment could extend survival. Patients with cancer who are depressed are often less adherent to oncology treatment and experience sleep and other circadian rhythm disruptions that can affect disease outcome (17). Depression among patients with cancer is a serious complicating comorbid illness and risk factor. Detection and treatment of depression is an important opportunity to improve the effectiveness of treatment.
Psychosocial Distress Screening Standard: Implementation
The standard states that when clinical evidence of moderate or severe distress exists, the oncology team (defined as the oncologist, nurse, social worker, and/or psychologist) is to identify physical, psychological, social, spiritual, and financial support needs and provide a link to services on-site or through referral. Oncology team members are advised to maintain a resource list to locate internal hospital psychiatrists, psychologists, and pastoral care providers. The network of psychosocial resources can be greatly expanded through integrating resources in the local community, such as Cancer Support Community sites, and nationally (e.g. American Cancer Society, CancerCare, LIVESTRONG). Academic and high-volume cancer centers may have greater access to on-site psychosocial care providers through integrating psychosocial providers as members of the oncology care team. The challenge for these settings is to manage volume, specifically with regard to distress screening administration and triage. Advances in health informatics and technology provide unparalleled opportunities to conduct distress screening within high-volume practices and deliver tailored resources to patients immediately after the reporting of concerns. Examples of electronic screening programs have begun to populate the literature over the past few years.
Electronic screening programs exist in various stages of development, from pilot testing to full implementation, at multiple cancer centers in the United States. These programs may be disease-specific or relevant to all disease sites (18). In addition, at least one program is using electronic symptom management assessment outside of the United States. A comprehensive review of electronic patient-reported symptom assessment systems in oncology was recently published (19).
Using Advances in Measurement Science and Health Informatics to Implement Distress Screening
Some large cancer centers in the United States have applied advances in measurement science and health informatics to implement patient-reported outcomes (PROs) assessment with electronic medical record (EMR) integration to facilitate provider notification and psychosocial triage. National Institutes of Health (NIH)-funded advances in measurement science provide accurate and precise assessment through the Patient Reported Outcomes Measurement Information System (PROMIS) network (www.nihpromis.org). PROMIS computer adaptive testing (CAT) item banks use a computer algorithm to administer PRO items tailored to the patient's symptoms severity. Precise, reliable, and valid symptoms scores are generated, with 4 to 6 items per symptom, computer-scored, and bench-marked based on normative data from thousands of patients. Assessment consists of PROMIS CAT item banks to measure anxiety, depression, fatigue, pain, and physical function, administered through Assessment Center (20). Assessment also includes a checklist of emotional, practical, and informational concerns that can be addressed by social workers or a medical librarian.
The intent of the EMR-integrated screening was 2-fold. First, communication barriers are bypassed through collecting PROs before clinic visits. Second, this system can enhance provider efficiency because medical staff know which symptoms to target before any direct interactions with the patient. This affords providers more time to focus on symptoms treatment, rather than assessment. Last, through using the EMR to facilitate the assessment of depression and anxiety and provide triage and referral when clinically indicated, the program's efficiency is enhanced through connecting patients most in need of psychosocial care with the on-site team (21).
Perceived Availability of External and Internal Resources
The external resources most often mentioned were availability of emotional support from family and friends and informational support from the treating team. In terms of internal resources, women explained that their ability to successfully cope with the stressors they were facing determined whether they would then accept or refuse additional support.
Availability of External Resources: Central role of family and friend support
More than three-quarters of the women who refused a referral felt they had an extensive family and friend network that they could readily turn to for emotional (e.g. someone to talk to, someone who would listen) or practical support (e.g. help with household duties, organizing appointments). One participant in this study said "family is key and all you need". Many of these participants inferred that if this support was lacking, they might have been more inclined to accept the referral to the psychologist. Three-quarters of the women who accepted a referral mirrored this finding; they wanted to see the psychologist because they needed someone to listen to them as they openly talked about the challenges and stressors they were facing (22). The psychologist is seen as a "neutral" person, who "allows you to say things you normally would not" and could offer a "different perspective" on what was happening to the patient. Before accepting the referral to the psychologist, many of these women often found themselves ruminating about how they were feeling and what they were confronted with, and knew it would be more constructive if they could talk to someone else about it. Many of these women also felt isolated, and the psychologist became their sole source of emotional support. For others, the emotional support they were receiving from family and friends was described as "not what they needed", or they felt they "needed more". For instance, one woman said her friends made her feel "like an invalid", and that she thought that when talking to someone she did not know, she would "talk better"; that she had the freedom to be open and honest, and speak of her experience in a way she could not with friends and family (22).
Women who reported feeling stigmatized were also particularly reticent to turn to family or friends for emotional support. Although some women described an extended network of family and friends, the fear of burdening them meant that the patients hesitated to turn to them for emotional support, and preferred to rely on the psychologist.
Satisfaction with Support Received from Other Health Care Professionals
Experience with other members of the health care team also seemed, for approximately half of the participants, to play a role in whether they accepted the additional psychological support offered. Mainly, if health care professionals met participants' informational needs and addressed most physical or medical concerns, then participants trusted their core treating team and did not feel they needed support from additional health care professionals. In addition, women stated that if their health care professionals reassured them that in time "it would be better," they just accepted that the situation was difficult for the present time and did not think much else could be done. However, for those who did not feel that reassurance, and needed additional information, they valued an opportunity to consult with another member of their health care team who could potentially reassure them that they were "not alone" and normalize their experience.
Perceived Ability to Independently Manage Cancer-Related Challenges
Three-quarters of the women who refused one-on-one counseling highly valued "working through it [herself]". For some accepting psychological assistance meant "you can't cope with the situation" and was admitting a certain level of personal defeat, and they felt that, although they were confronted with several stressors, their situation was "not bad enough". Approximately half of these participants mentioned that they would be willing to see the psychologist if they felt their coping strategies were ineffective and the situation was getting worse (22). Common coping strategies these participants described included self-talk, "being positive," "preparing for the worst and hoping for the best," setting goals, trying not to dwell on the negativity of the situation, reframing, minimizing worries/anxieties, distraction (e.g. keeping busy, a lot of hobbies), relaxation techniques (e.g. deep breathing exercises), engaging in enjoyable activities (e.g. part of a social group), and participating in religious activities (e.g. praying). These coping strategies were often lifelong skills that had been used during other stressful life events and were transferable to current challenges.
Conversely, women who sought counseling often spoke of needing more information on how best to take care of themselves and cope with their overwhelming emotions and worries and the losses they were facing. Some women had tried to cope with the situation, but they felt they just did not have the skills to efficiently and effectively cope with the stressors they were facing. Many spoke of the intensity of the whirlwind of cancer, which had "robbed" them of any internal resources they had (e.g. independence), and described feeling little control over the situation and like their ability to cope was "completely depleted". Thus, usual approaches to coping with life stressors were not applicable or useful, and these women decided to "get help" (22).
PROGRESS FOR DISTRESS MANAGEMENT IMPLEMENTATION
There has been growing recognition in recent years that psychosocial care is an important component of the comprehensive care of people diagnosed with cancer. Despite evidence of the effectiveness of psychosocial services, many patients do not receive help for problems that would benefit from this type of care (e.g. emotional and practical problems). To address this issue, the recommendations that standards for the quality of cancer care include the provision of appropriate psychosocial health services. Toward this end, the recommendations outline a model for the delivery of care in which processes are in place to identify patients' psychosocial health needs and link them with needed services. Current survey suggested routine screening for distress as part of clinical care seems to have been more widely implemented over time (23). This change is evidenced by the increase from 53% in 2005 to 60% in 2012 in the percentage of institutions that conduct any routine outpatient screening. Most of this change reflects an increase in the percentage of institutions in United States reporting that all outpatients are screened routinely (20% in 2005 vs. 30% in 2012). The percentage of institutions reporting that they only screen specific subgroups of outpatients has remained relatively constant (33% in 2005 vs. 30% in 2012). The current survey also found that 36% of institutions are screening some or all inpatients for distress. The finding that 79% of institutions that screen for distress subsequently rescreen patients also indicates an increased awareness of the value of screening. The variety of intervals and frequencies reported indicates that no standardized approach yet exists for when and how often patients are rescreened (23).
Consistent with the growing evidence regarding the usefulness of brief screening measures in identifying clinically significant distress, the use of these measures seems to have gained greater acceptance over time (24). Distress thermometer is the most commonly used self-report measure among institutions performing any screening. Findings from current survey also suggest the increased use of emerging technologies to facilitate screening and referral practices. Although most institutions using self-report measures administer them via paper and pencil, nearly as many institutions are using tablet or Web-based applications in place of or in addition to paper and pencil administration. Additionally, 14% of institutions are now triaging distressed patients using automated processes to generate a referral. Although informative, the current survey and comparisons with the previous survey have several limitations. First, some institutions did not participate in one or both of the surveys. Although high rates of participation findings were achieved (83% in 2005 and 91% in 2012), findings should be considered representative only of the subset of institutions that provided responses. Second, because of changes in membership and variability in which institutions completed the 2005 and 2012 surveys, the comparisons reported do not reflect changes over time at the same set of institutions. Third, the limited number of member institutions precludes conducting meaningful statistical comparisons of changes over time. Fourth, the responses obtained correspond to the views of the institutional representative who completed the survey (23). Whether an on-site audit of screening practices at each institution would yield similar results remains unknown.
RESEARCH IMPLICATIONS
Additional studies are needed to further examine, on a large scale, patients' preferences for follow-up care after distress screening. Several different approaches to distress screening are discussed above, and additional studies should examine their comparative acceptability and efficacy. One particularly promising avenue for future research is to evaluate a stepped approach to care. Although this model of care has long been advocated in cancer care and seems particularly promising in light of the findings of these studies, few studies have examined its appropriateness and efficacy among patients with cancer. Moreover, examining the acceptability of combining the DT with other thermometers to measure key concepts that emerged from this study (e.g. a "social support thermometer") is another potential focus for futures research. Based on the finding that many women preferred to self-manage their distress, more research is needed to determine the kind of services these women would deem more acceptable to help them in their coping efforts.
SUMMARY
Given that the popularity of distress screening is increasing exponentially, and begins to bridge the gap between clinicians' and patients' expectations of how psychosocial services should be used in response to distress screening. Key findings and implications for service delivery were: 1) receptivity to referral is a separate issue from that of distress level, 2) strong preference among those who declined psycho-oncology referral to cope on their own emphasized the potential role of self-management interventions, and 3) low social support was a major theme among those accepting referral, suggesting that assessing family support might further contribute to identifying patients in need of additional psychological assessment.
Psychosocial oncology clinicians and researchers have had a long-standing interest in the implementation of distress screening and are eager to partner with cancer care settings on these efforts. The emerging accreditation standards offer an unparalleled opportunity to apply the science of psychosocial care in clinical practice. The mandate is to use implementation science to maximize outcomes for patients. Through doing so, the quality of cancer survivorship can be improved dramatically. Greater progress can be seen in the use of self-report measures as part of screening, with a 23% increase since 2005 in the use of these measures alone or in combination with and interview. A major impetus for additional progress will be the standards for patient-centered-care that were issued in 2011 by the American College of Surgeons Commission on Cancer, a body that accredits more than 1,500 hospitals in the United States. Among the new standards is one specifying that local oversight committees develop and implement processes for psychosocial distress screening and referral for the provision of psychosocial care. Plans to monitor for compliance with these standards as part of the accreditation process should provide strong motivation to complete the implementation of elements of Distress Management related to distress screening and care of distressed patients.
Among the new standards is one specifying that local oversight committee develop and implement processes for psychosocial distress screening and referral for the provision of psychosocial care. Plans to monitor compliance with these standards as part of the accreditation process should provide strong motivation for the member institutions and others to complete the implementation of elements of the guidelines for distress management related to distress screening and care of distressed patients.
References
- Holland JC, Andersen B, Britbart WS, et al. NCCN Clinical Practice Guidelines in Oncology: Distress Management. Version 2, 2013. Available at www.NCCN.org Accessed on 14 October 2014
- Carlson LE, Waller A, Mitchell AJ. Screening for distress and unmet needs in patients with cancer: review and recommendations. J Clin Oncol 2012;30:1160-1177
- Shimizu K, Ishibashi Y, Umezawa S, et al. Feasibility and usefulness of the 'Distress Screening Programs in Ambulatory Care' in clinical oncology practice. Psychooncology 2010;19:718-725
- Jacobsen P. Promoting evidence-based psycho-social care for cancer patients. Psychooncology 2009;18:6-13
- Gessler S, Low J, Danielle E, et al. Screening for distress in cancer patients: is the distress thermometer a valid measure in the UK and does it measure change over time? A prospective validation study. Psychooncology 2008;17:538-547
- Low J, Gessler S, Williams R, et al. Screening for distress and depression in cancer patients: is ultra-short depression screening a valid measure in the UK? A prospective validation study. J Pain Symptom Manage 2009;38:234-243
- Boyes A, D'Este C, Carey M, et al. How does the Distress Thermometer compare to the Hospital Anxiety and Depression Scale for detecting possible cases of psychological morbidity among cancer survivors? Support Care Cancer 2012;1:1-9
- American College of Surgeons Commission on Cancer. Cancer Program Standards 2012, Version 1.1: Ensuring Patient-Centered Care. Available at: www.facs.org/cancer/coc/programstandards2012.html Accessed January 22, 2015
- Giese-Davis J, Collie K, Rancourt KM, et al. Decrease in depression symptoms is associated with longer survival in patients with longer survival in patients with metastatic breast cancer: a secondary analysis. J Clin Oncol 2011;29:413-420
- Carlson LE, Waller A, Mitchell AJ. Screening for distress and unmet needs in patients with cancer: review and recommendations. J Clin Oncol 2012;30:1160-1177
- Johnson TV, Garlow SJ, Brawley OW, et al. Peak window of suicides occurs within the first month of diagnosis: implications for clinical oncology. Pscychooncology 2012;21:351-356
- Kessler RC, Petukhova M, Sampson NA, et al. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int J Methods Psychiatr Res 2012;21:169-184
- Miller AH, Ancoli-Israel S, Bower JE, et al. Neuroendocrine-immune mechanisms of behavioral comorbidities in patients with cancer. J Clin Oncol 2008;26:971-982
- Akechi T, Okuyama T, Onichi J, et al. Psychotherapy for depression among incurable cancer patients. Cochorane Database Syst Rev 2008;CD005537
- Cohen K, Cole SW, Sood AK, et al. Depressive symptoms and cortisol rhythmicity predict survival in patients with renal cell carcinoma: role of inflammatory signaling. PLos One 2012;7:e42324
- Spiegel D. Mind matters in cancer survival. JAMA 2011;305:502-503
- Manning M, Bettencourt BA. Depression and medication adherence among breast cancer survivors: bridging the gap with the theory of planned behavior. Psychol Health 2011;26:1173-1187
- Carlson LE, Groff SL, Bultz BD, et al. Online screening for distress, the 6th vital sign, in newly diagnosed oncology outpatients: Randomized controlled trial of computerized vs personalized triage. Br J Cancer 2012;107:617-625
- Bennett AV, Basch E, Jensen RE. Electronic patient-reported outcome systems in oncology clinical practice. CA Cancer J Clin 2012;62:336-347
- Gershon R, Rothrock NE, Hanrahan RT, et al. The development of a clinical outcomes survey research application: Assessment Center. Qual Life Res 2010;19:677-685
- Wagner LI, Spiegel D, Pearman T. Using the science of psychosocial care to implement the new American college of surgeon commission on cancer distress screening standard. JNCCN 2013;11:214-221
- Lambert SD, Kelly B, Boyes A, et al. Insights into preferences for psycho-oncology services among women with gynecologic cancer following distress screening. J Natl Compr Canc Netw 2014;12:899-906
- Wagner LI, Spiegel D, Pearman T. Using the science of psychosocial care to implement the new American College of Surgeons Commission on Cancer Distress screening standard. JNCCN 2013;11:214-221
- Carlson LE, Waller A, Mitchell AJ. Screening for distress and unmet needs in patients with cancer: review and recommendations. J Clin Oncol 2012;30:1160-1177
Published: 17 February 2015
Dedicated to Women's and Children's Well-being and Health Care Worldwide
www.womenshealthsection.com